Earl came to our first session with a question he had been turning over for months. His daughter had told him to cut sugar because it was inflammatory, and he wanted to know if it would actually help his knees. So does sugar cause knee pain, or was his daughter overstating it?
The honest answer sits in the middle. Sugar does not directly cause knee pain, but research on adults over 55 shows added sugar raises inflammation and is linked to higher osteoarthritis risk. For adults already managing knee pain, that link matters.
Key Takeaway
Does sugar cause knee pain? Research links added sugar intake to higher osteoarthritis risk in adults (Liao et al., 2024). In controlled feeding trials, sugar-containing foods raised inflammatory biomarkers (Qi et al., 2022). For adults over 55 managing joint pain, reducing added sugar is one lever that may matter.
If you have wondered “does sugar cause knee pain,” this post covers what research shows about sugar and joints, how much actually matters, and simple shifts that work for adults over 55.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
Does sugar cause knee pain in adults over 55?
Short answer: not directly. No study has shown a spoonful of sugar reaching your knee and creating pain. What the research actually shows is a link between added sugar intake and a higher risk of osteoarthritis over time.
A 2024 case-control study used NHANES data from over 10,000 US adults. Researchers found that higher added sugar intake was associated with greater osteoarthritis risk (Liao et al., 2024). The link was stronger in women, in adults with lower BMI, and in those without diabetes.
So when people ask whether sugar causes knee pain, the clean answer is this. Sugar is not the only factor, but for adults over 55 already dealing with joint issues, added sugar is one piece worth looking at.
How does sugar affect inflammation and joint pain?
Sugar does not attack your joints directly. It works through inflammation.
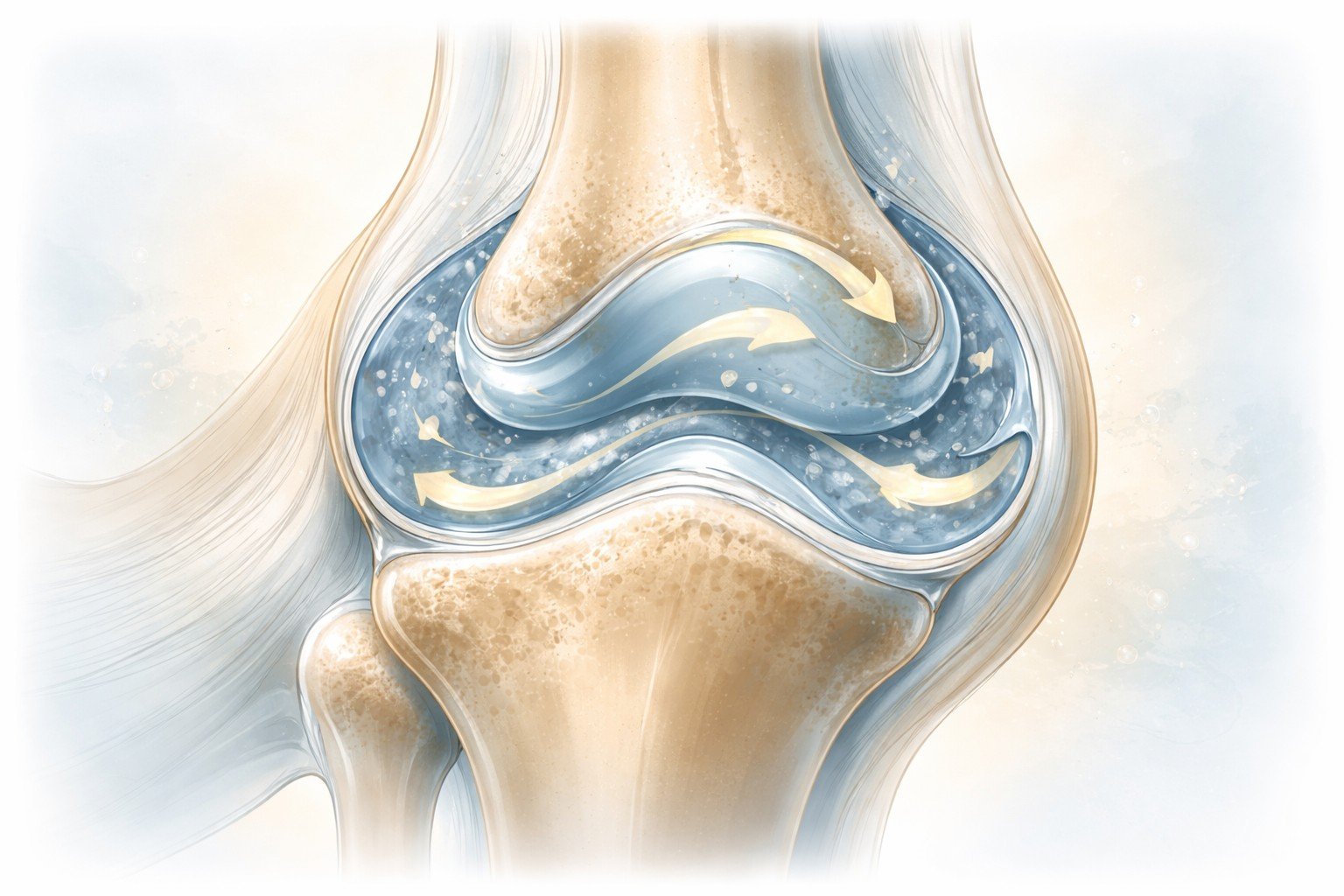
When you eat added sugar, your body produces more inflammatory signals. A 2022 systematic review pooled controlled feeding trials in humans and found that sugar-containing beverages raised levels of C-reactive protein (CRP), a marker of inflammation (Qi et al., 2022). For adults over 55, that matters. Cartilage and joint tissue get more sensitive with age, and higher background inflammation adds to wear already happening in the knee.
This is the real mechanism people ask about when they wonder whether sugar causes knee pain. Sugar does not cause the pain itself, but it raises inflammation, and inflammation makes joint pain harder to manage.
How much sugar is too much for joint health?
There is no perfect number for everyone. The American Heart Association suggests a daily cap of about 6 teaspoons of added sugar for women and 9 teaspoons for men. That is a useful starting point, not a strict rule.
For adults over 55 asking does sugar cause knee pain, the more useful question is where your sugar is coming from. Added sugar in sodas, sweetened coffee, and packaged snacks hits the bloodstream fast and drives inflammation. The natural sugar in whole fruit comes with fiber that slows absorption and antioxidants that help. The two are not the same.
Most adults underestimate their intake. A single 20-ounce soda is about 16 teaspoons of added sugar, almost double the daily cap on its own.
What foods raise inflammation for adults over 55?
Sugar is not the only driver. Inflammation responds to the full food pattern.
The foods most consistently linked to higher inflammation in adults include sugary drinks, refined grains, processed meats, and fried foods. When these take up most of a daily diet, inflammatory markers stay elevated.
The flip side is just as real. A 2024 study of over 10,000 US adults found that higher added sugar intake was linked to greater frailty, meaning reduced strength and function in daily life (Ji et al., 2024). For adults wondering, does sugar cause knee pain, this is the broader picture. Sugar affects not just joints but also what your body can do.
How can adults over 55 reduce sugar without giving up everything?
Going all-or-nothing is the fastest way to quit a change. Small shifts work better.
Start with one category. If sugary drinks are in your day, switch one for water, sparkling water, or unsweetened tea. That single change often drops daily added sugar by 20 to 40 grams with almost no effort.
Next, read one label a day. Pick a food you eat often and look at the added sugars line. You are not trying to eliminate sugar. You are building awareness of where it hides.
For adults over 55 wondering does sugar cause knee pain enough to change how they eat, the answer is not perfection. It is lowering the overall load. A small daily shift, held for 90 days, moves the needle.
If you have diabetes, insulin resistance, or other conditions affected by diet, check with your doctor before making significant changes.
Wrap-up: Does sugar cause knee pain?
Sugar does not cause knee pain on its own, but it raises inflammation, and inflammation makes joint pain harder to manage for adults over 55. Research links added sugar to greater osteoarthritis risk and to reduced strength and function in daily life.
The path forward is not a restrictive diet. It is awareness, one swap at a time, held long enough to matter.
Does sugar cause knee pain is one piece of a larger picture. If you want the full approach, the complete guide to knee pain relief for adults over 55 is the place to start.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Frequently Asked Questions
Can cutting sugar reduce knee swelling?
Lowering added sugar can reduce general inflammation, which may help with visible joint swelling over weeks or months. Results are usually not dramatic or immediate. If swelling is sudden, hot, or paired with fever, that is not a sugar issue. Have it checked by your doctor promptly.
How quickly will cutting sugar improve knee pain?
Most adults see a measurable shift in inflammation markers within 2 to 6 weeks of sustained change. Felt improvement in joint comfort often takes 6 to 12 weeks. If you are asking, does sugar cause knee pain and want relief fast, build your change on consistency, not intensity.
Does sugar affect all types of knee pain equally?
No. Sugar most affects knee pain tied to inflammation or osteoarthritis. Pain from a recent injury, ligament damage, or meniscus tear responds more to rest, movement, and sometimes surgery than to diet. When people ask does sugar cause knee pain, the answer applies most to chronic inflammatory conditions.
Which hidden sources of sugar affect adults over 55 the most?
The biggest hidden sources are flavored yogurts, breakfast cereals, pasta sauces, salad dressings, and sweetened coffee drinks. Many “healthy” products marketed to adults over 55 contain more added sugar than a standard cookie. Reading the added sugars line on the label is the fastest way to spot them.
Should I replace sugar with artificial sweeteners?
That is a personal call. Artificial sweeteners cut added sugar without calories, but research on their long-term health effects is mixed. Natural non-caloric options like stevia and monk fruit have a cleaner track record in current studies. Water, unsweetened tea, and sparkling water remain the safest bets.
Does honey or agave count as added sugar?
Yes. Honey, agave, maple syrup, and coconut sugar are all added sugars. They raise blood sugar and inflammatory signals much like table sugar does. The “natural” label does not change the physiological effect. For joint inflammation, the body responds to the sugar, not the source.
Ji, J., Qiu, J. F., Tao, Y., Xu, M., Pei, B., Wu, C., Huang, G., & Qian, D. (2024). Association between added sugars and frailty in U.S. adults: A cross-sectional study from the National Health and Nutrition Examination Survey 2007–2018. Frontiers in Public Health, 12, 1403409. https://doi.org/10.3389/fpubh.2024.1403409
Liao, X., Chen, X., Zhou, Y., Xing, L., Shi, Y.-H., & Huang, G. (2024). Added sugars and risk of osteoarthritis in adults: A case-control study based on National Health and Nutrition Examination Survey 2007–2018. PLoS ONE, 19(11), e0313754. https://doi.org/10.1371/journal.pone.0313754
Qi, X., Chiavaroli, L., Lee, D., Ayoub-Charette, S., Khan, T. A., Au-Yeung, F., Ahmed, A., Cheung, A., Liu, Q., Glenn, A. J., Blanco Mejia, S., Rahelić, D., Kahleová, H., Salas-Salvadó, J., Kendall, C. W. C., & Sievenpiper, J. L. (2022). Effect of important food sources of fructose-containing sugars on inflammatory biomarkers: A systematic review and meta-analysis of controlled feeding trials. Nutrients, 14(19), 3986. https://doi.org/10.3390/nu14193986
Maureen showed up to our first call exhausted. She told me her knees were fine most afternoons, and then 2 am would break her. Knee pain worse at night is common in adults over 55, and it has real physiological drivers.
The ache would show up right when her body should have been at rest. She would end up staring at the ceiling for another forty-five minutes. If this sounds familiar, you are not alone.
Research on older adults with knee osteoarthritis shows nighttime pain is genuinely higher than daytime pain. There are real reasons for this, and real things that help.
Key Takeaway
Most adults over 55 experience knee pain worse at night compared to during the day (van Berkel et al., 2023). In a study of 1,214 adults, nocturnal knee pain rose from 3.6% in those with no osteoarthritis to 75% in those with severe osteoarthritis (Sasaki et al., 2014). Behavioral changes reduce the disruption.
This post covers why knee pain worsens at night, the sleep positions that reduce it, the evening habits that help, and what to do when pain wakes you up.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
Is it normal for knee pain to get worse at night?
Short answer: yes, for most adults over 55 with osteoarthritis. In a large Japanese study of 1,214 adults with an average age of 58, researchers found that nocturnal knee pain showed up in about 1 in 5 people with mild osteoarthritis and in 3 out of 4 people with severe osteoarthritis (Sasaki et al., 2014).
A Dutch study found the same pattern. Three out of four adults with hip or knee osteoarthritis reported pain at night, and they rated that pain higher than their daytime pain (van Berkel et al., 2023).
If your knees wake you up when you are trying to sleep, you are not imagining it. This matches what a lot of us experience with knee pain worse at night.
Why is knee pain worse at night after 55?
Three factors stack up at night.
The first is inflammation. A large study of 1,002 adults with early hip or knee pain found that higher blood markers of inflammation were linked to both the presence of nocturnal pain and its worsening over two years (van Berkel et al., 2022). Inflammation in the joint does not take a break when you do.
The second is reduced daytime distraction. During the day, your attention is pulled in a dozen directions. At night, the house is quiet, and your knee has the floor.
The third is joint wear that builds up after 55. Cartilage thins, and the tissue around the joint gets more sensitive. The same irritation you could ignore at 40 now keeps you awake. Knee pain worse at night tracks closely with how advanced the osteoarthritis is (Sasaki et al., 2014).
What is the best sleeping position for knee pain?
For most adults over 55 with sore knees, side sleeping with a pillow between the knees is the most comfortable position. The pillow keeps your top knee from pressing down on your bottom knee and keeps your hips in a neutral line.
If you sleep on your back, try a pillow under your knees. A small lift takes pressure off the joint and lets the muscles around the knee relax.
Stomach sleeping is the one to avoid. It twists the knees outward and keeps them flat against the mattress all night. Most physical therapists will tell you the same thing.
Your position at night is one of the simplest levers you have when knee pain is worse at night and is keeping you up. A supportive mattress matters too. One that is too soft lets your knees sag out of alignment.
What evening habits help knee pain worse at night?
A few simple habits in the hour before bed make a real difference.
The first is a gentle movement earlier in the evening. A short walk after dinner keeps the joint fluid moving and the muscles around the knee from stiffening up. The same pattern that helps with morning knee stiffness also helps at night.
The second is warmth. A warm bath about an hour before bed relaxes the tissue around the joint.
The third is a quiet wind-down. A research team followed 100 adults with knee osteoarthritis through a behavioral sleep program. Better sleep continuity, not pain reduction, shifted how they experienced pain (Lerman et al., 2017).
Keep screens dim after 9 pm and the bedroom cool. Stacked together, these habits move the needle when knee pain is worse at night and keeps you up.
What should you do when knee pain wakes you up?
Pain at 3 am pulls you out of deep sleep fast. The more you lie there fighting it, the more wound up your nervous system gets.
First, shift your position. If you are on your back, roll to your side with a pillow between your knees. If you are already on your side, flip to the other side. The joint has been loaded in one position for hours, and changing that often takes the edge off.
If shifting does not work, get up for a few minutes. Walk slowly to the bathroom. A gentle 90 seconds of movement resets the joint without waking you fully.
Skip the phone. Blue light will cost you another forty-five minutes. A calm position change handles knee pain worse at night better than powering through it.
Wrap-up: Why knee pain gets worse at night (and what actually helps)
Nighttime knee pain is real, and research points to why it happens. Inflammation does not clock out when you do, daytime distractions fall away, and the joint wear that builds up after 55 makes the whole system more sensitive.
The good news is that what helps is also behavioral. A better sleep position. A pillow between the knees. Gentle evening movement. A calm wind-down hour. A quiet response when pain wakes you up at 3 am.
Knee pain worse at night is one piece of a larger picture. If you want to understand the full approach, the complete guide to knee pain relief for adults over 55 is the place to start.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Frequently Asked Questions
Is ice or heat better for knee pain before bed?
Heat works better for most adults with nighttime knee pain. A warm compress or heating pad for 15 to 20 minutes before bed relaxes the muscles around the joint and helps you settle. Use ice only if the knee is visibly swollen or if you have had recent activity that flared it up.
Can gentle stretching before bed help knee pain?
Yes, short and easy stretches help. A 2-minute sequence of ankle circles, seated hamstring stretches, and slow knee bends eases the tissue around the joint before sleep. Keep the stretches light. Anything that sharpens the pain should stop. The point is to calm the area, not challenge it.
Does nighttime knee pain mean my arthritis is getting worse?
Not always. Pain intensity at night does track with osteoarthritis severity in population studies, but a rough night on its own does not mean your arthritis has progressed. Many adults with steady arthritis experience knee pain worse at night due to inflammation cycles. Talk to your doctor if the trend is one-way over weeks.
How long before I see improvement in nighttime knee pain?
Most adults notice some difference within 2 to 3 weeks of consistent changes. Sleep position and evening habits tend to show earlier. Broader shifts in knee pain, worse at night, usually take 6 to 12 weeks because tissue sensitivity and sleep patterns both need time to reset. Steady wins over dramatic.
Why does knee pain sometimes feel different at night than during the day?
Nighttime pain often has a deeper, steadier ache compared to the sharper mechanical pain of daytime use. Research on hip and knee osteoarthritis patients shows nighttime pain tends to be more constant, with higher worst-pain scores than daytime. The nervous system runs on different settings at night, which changes how pain is registered.
When should you see a doctor about knee pain that wakes you up?
See a doctor if knee pain is worse at night and is paired with visible swelling, redness, warmth, fever, sudden weakness, or pain that keeps intensifying over several weeks. A knee that locks or gives out is also worth a visit. Most nighttime knee pain is manageable with behavioral changes, but these specific signs need a clinical look.
References
Lerman, S. F., Finan, P. H., Smith, M. T., & Haythornthwaite, J. A. (2017). Psychological interventions that target sleep reduce pain catastrophizing in knee osteoarthritis. Pain, 158(11), 2189–2195. https://doi.org/10.1097/j.pain.0000000000001023
Sasaki, E., Tsuda, E., Yamamoto, Y., Maeda, S., Inoue, R., Chiba, D., Okubo, N., Takahashi, I., Nakaji, S., & Ishibashi, Y. (2014). Nocturnal knee pain increases with the severity of knee osteoarthritis, disturbing patient sleep quality. Arthritis Care & Research, 66(7), 1027–1032. https://doi.org/10.1002/acr.22258
van Berkel, A. C., Ringelenberg, R., Bindels, P. J. E., Bierma-Zeinstra, S. M. A., & Schiphof, D. (2023). Nocturnal pain, is the pain different compared with pain during the day? An exploratory cross-sectional study in patients with hip and knee osteoarthritis. Family Practice, 40(1), 75–82. https://doi.org/10.1093/fampra/cmac074
van Berkel, A. C., van Spil, W. E., Schiphof, D., Runhaar, J., van Ochten, J. M., Bindels, P. J. E., & Bierma-Zeinstra, S. M. A. (2022). Associations between biomarkers of matrix metabolism and inflammation with pain and fatigue in participants suspected of early hip and or knee osteoarthritis: Data from the CHECK study. Osteoarthritis and Cartilage, 30(12), 1640–1646. https://doi.org/10.1016/j.joca.2022.08.013
A client told me last month she had bought three pairs of walking shoes in six months. Each time her knees felt better for a week, then worse again. The shoe was not the answer, and the research agrees.
She was sure the fix was on a shelf somewhere. The right cushioning. The right brand. For her, walking shoes and knee pain were a shopping problem.
I hear this every week. Adults over 55 trying to figure out walking shoes and knee pain almost always start with the shoe. It makes sense. The shoe is the part you can swap out today. Your body is not.
What I see in clients’ lines up with what the studies show. Shoes matter less than most adults think.
Key Takeaways
Walking shoes affect how your knees feel during walking, but much less than most adults believe. A 2025 study found that walkers perceived clear differences between supportive and flexible footwear, while their actual movement showed no significant change (Katugam-Dechene et al., 2025). The honest truth on walking shoes and knee pain is that what you feel in a shoe and what your body does in it are often two different things.
The rest of the post lays out the research, what walking shoes can and cannot do for knee pain, and a simple way to tell if your shoes or your body is driving the discomfort. discomfort.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
Why do most adults blame their shoes first?
Because the shoe is the variable you can change today.
You can swap out a shoe in an afternoon. You can read reviews and feel like you are doing something about the knee pain. The body underneath the shoe is harder to think about, and much harder to change.
Marketing knows this. Every walking shoe ad tells you the right pair will change how you feel. And a new shoe does feel different for the first few walks.
Here is where it gets interesting. In a 2025 study, adults completed walking tasks in two very different shoes: a supportive hiking boot and a flexible sneaker. Walkers reported clear differences between the two. Their actual movement data showed almost none (Katugam-Dechene et al., 2025).
The shoe feels different. The body does what it was going to do anyway. This is the core of the research on walking shoes and knee pain. What you feel is not what your body does.
What do walking shoes actually do for knee pain?
Less than most adults hope. More than nothing. That is the summary on walking shoes and knee pain.
Shoes change how force travels through your knee. They shift where the load lands and how your leg muscles respond. The right shoe nudges these things in a better direction. The effect is real, but small.
One study shows the ceiling plainly. Researchers designed a variable-stiffness shoe for one purpose: to reduce knee load in adults with medial compartment knee osteoarthritis. Engineers who understood the biomechanics built it from the ground up. The result was a reduction in the knee adduction moment of about 7 percent (Jenkyn et al., 2011).
A follow-up tracked the same shoes over six months in patients with knee pain. Pain scores and function improved, but the gains were modest, and the control group also saw some improvement (Erhart et al., 2010).
That is the honest answer on walking shoes and knee pain. Shoes help a little. They do not fix what is happening underneath.
Can the wrong walking shoes make knee pain worse?
Yes. This is the honest counterweight to walking shoes and knee pain.
A 2021 study measured joint loads directly during walking using instrumented hip prostheses. Shoes with very stiff soles or elaborate cushioning increased hip joint loads compared to barefoot walking (Palmowski et al., 2021). Expensive and supportive does not automatically mean better for painful joints.
Researchers tested shoe features for balance in adults. Their recommendation after comparing soft soles, elevated heels, raised collars, and tread patterns was simple: a standard laced shoe with a low collar and a standard sole hardness (Menant et al., 2008). The fancy features did not help. Several made the balance worse.
Shoe wear matters too. Worn-out shoes change how your leg muscles stabilize your knee during walking (Jafarnezhadgero et al., 2020). If your knees hurt in an older pair, the answer may not be a fancier new pair. It may be any reasonable shoe that fits and is not broken down.
When clients ask about walking shoes and knee pain, this is where the conversation lands. Less is often more.
When should you actually replace your walking shoes?
Between 300 and 500 miles, or about every six months, for daily walkers. A worn shoe is often the real driver of walking shoes and knee pain troubles.
The research gives a reason beyond the odometer. Studies tracking shoe use over six months show measurable changes in shoe stiffness and in the muscle co-contraction patterns your body uses to stabilize your knee and ankle during walking (Jafarnezhadgero et al., 2021). Your shoes are not the same at month six as they were at month one.
Three quick checks if you are wondering whether your shoes are done. Look at the outsole for smooth, worn patches where the tread used to be. Press the midsole with your thumb. If it stays compressed, the cushioning is gone.
Then check the flex point at the ball of the foot. A shoe that folds easily in the middle instead is past its life. That folding test alone catches a lot of worn shoes, and it can be one real reason adults over 55 struggle with walking shoes and knee pain in an older pair.
How do you know if your shoes are the problem or your body is?
You test it.
If your shoes are driving the discomfort, changing shoes or changing how you walk should change how your knees feel. If your shoes are not the main factor, your knees will respond to how you walk, not to what you wear.
That is what the Walk Test is for. It is a short three-day check that uses a simple walking pattern most adults over 55 can do in their own neighborhood. The test is not about your shoes. It is about what your body can do when you give it a specific kind of walk.
Three days is long enough to see a pattern. Short enough that you will not give up on it.
If your comfort changes across the three days, you have an answer. You have also learned something about walking shoes and knee pain that no shoe review can tell you. The answer to walking shoes and knee pain is about your body, not about your shoes. That is where any real solution starts.
Wrap-up: Walking shoes and knee pain after 55
The short version is this. Shoes matter, but less than most adults think. Even shoes engineered specifically to reduce knee load change joint forces by modest amounts. Too much cushioning or stiffness can work against you.
A worn-out shoe changes how your body moves, which is a better reason to replace shoes than any brand recommendation. If you have been asking which walking shoe will solve your knee pain, the better question is what your body is doing when you walk. For the structural side, the post on why your knees hurt when you walk covers what is happening underneath.
Walking shoes and knee pain are one piece of a larger picture. For the full approach to knee pain relief for adults over 55, the complete guide is the place to start.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Frequently Asked Questions
Are cushioned shoes or supportive shoes better for knee pain after 55?
The research is mixed, but newer evidence leans toward supportive over cushioned. A 2019 Australian trial of 164 adults over 50 with knee osteoarthritis found that 58 percent of participants wearing sturdy supportive shoes reported meaningful pain reduction, compared to 40 percent wearing flat flexible shoes (Paterson et al., 2019). For adults facing walking shoe and knee pain choices, support tends to outperform cushion alone.
Are running shoes better than walking shoes for knee pain after 55?
Not for most adults. Running shoes are built for repeated high-impact landings, which means stiffer heels and more aggressive forefoot geometry than your walking stride needs. A well-fitted walking shoe or a neutral athletic shoe usually feels better during long walks. Running shoes can work if they fit your foot and feel comfortable for your pace.
Do rocker-bottom shoes help with knee pain when you walk?
Sometimes. Rocker-bottom shoes shift how your foot rolls through each step, which can reduce load on the knee for some walkers. Research on specialized rocker designs found modest benefits similar to standard walking shoes. If a rocker bottom feels more comfortable during a full walk, it may be worth trying. If not, a standard walking shoe works fine.
Why do your knees hurt more after walking on hard surfaces?
Hard surfaces return more force to your joints with each step. Concrete and asphalt give you almost no give, so your shoes and your body absorb everything. Softer surfaces like grass, dirt paths, and rubberized tracks cushion the impact. If your usual walking route is all sidewalks, adding even one softer-surface walk per week can reduce cumulative strain.
How do you break in new walking shoes if your knees already hurt?
Start with short walks of 10 to 15 minutes for the first three or four days. New shoes change how force travels through your legs, and your muscles need time to adapt. If your knees feel worse after a new pair for more than two weeks of regular use, the fit may be wrong for your foot. A specialty walking store can help you check.
How do you break in new walking shoes if your knees already hurt?
Start with short walks of 10 to 15 minutes for the first three or four days. New shoes change how force travels through your legs, and your muscles need time to adapt. If your knees feel worse after two weeks of regular use, the fit may be wrong. A specialty walking store can help you check.
References
Erhart, J. C., Mündermann, A., Elspas, B., Giori, N. J., & Andriacchi, T. P. (2010). Changes in knee adduction moment, pain, and functionality with a variable-stiffness walking shoe after 6 months. Journal of Orthopaedic Research, 28(7), 873–879. https://doi.org/10.1002/jor.21077
Jafarnezhadgero, A. A., Anvari, M., & Granacher, U. (2020). Long-term effects of shoe mileage on ground reaction forces and lower limb muscle activities during walking in individuals with genu varus. Clinical Biomechanics, 73, 55–62. https://doi.org/10.1016/j.clinbiomech.2020.01.006
Jafarnezhadgero, A. A., Piran Hamlabadi, M., Anvari, M., & Zago, M. (2021). Long-term effects of shoe mileage on knee and ankle joints muscle co-contraction during walking in females with genu varus. Gait & Posture, 89, 74–79. https://doi.org/10.1016/j.gaitpost.2021.07.004
Jenkyn, T. R., Erhart, J. C., & Andriacchi, T. P. (2011). An analysis of the mechanisms for reducing the knee adduction moment during walking using a variable stiffness shoe in subjects with knee osteoarthritis. Journal of Biomechanics, 44(7), 1271–1276. https://doi.org/10.1016/j.jbiomech.2011.02.013
Katugam-Dechene, K., Cook, A., Nguyen, A., Smith, R., Shelton, A., & Franz, J. R. (2025). The effects of shoe structural features on agility and stability tasks during walking. PeerJ, 13. https://doi.org/10.7717/peerj.19930
Menant, J. C., Perry, S. D., Steele, J. R., Menz, H. B., Munro, B. J., & Lord, S. R. (2008). Effects of shoe characteristics on dynamic stability when walking on even and uneven surfaces in young and older people. Archives of Physical Medicine and Rehabilitation, 89(10), 1970–1976. https://doi.org/10.1016/j.apmr.2008.02.031
Palmowski, Y., Popović, S., Kosack, D., & Damm, P. (2021). Analysis of hip joint loading during walking with different shoe types using instrumented total hip prostheses. Scientific Reports, 11(1), 10073. https://doi.org/10.1038/s41598-021-89611-8
If you have ever dragged yourself out of bed and spent the first ten minutes of your morning wondering if your knees were going to cooperate, you already understand morning knee stiffness causes and relief better than most doctors explain it. That slow, grinding warmup is not random. It has a reason. And once you know the reason, the fix makes complete sense.
If you recognize that feeling, you already know what morning knee stiffness causes and what relief looks like in practice. You learn your pattern. You take it slow. You wait for your body to catch up with the day.
But here is what most people do not know about why it happens.
KEY TAKEAWAY
Morning knee stiffness is caused by synovial fluid, your knee joint’s natural lubricant, thickening during sleep from hours of inactivity. Movement redistributes that fluid and reduces stiffness faster than rest. In adults with knee osteoarthritis, morning stiffness that resolves in less than 30 minutes with activity is a recognized clinical pattern, not a sign that something is getting worse (Duong et al., 2023).
Here is what is actually happening inside the joint, how long morning stiffness should last, and the one thing that helps most.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
Why do knees get so stiff overnight?
Your knee joint sits still for six to eight hours while you sleep, with very little movement to keep things circulating. The synovial fluid inside the joint, which normally acts as a lubricant between surfaces, thickens when it is not being moved through. Think of it like a jar of honey left in a cold kitchen overnight. It is still there. It just does not flow the way it did the day before.
That thickening is what creates the morning knee stiffness causes and relief pattern so many adults over 55 know well. The joint needs movement to warm that fluid back up and redistribute it across the cartilage surfaces. Without that movement, the first steps of the day feel stiff, slow, and sometimes a little unpredictable.
The good news is that the fix is built right into the problem. Movement is both the cause of relief and the trigger for it.
What is actually happening inside the joint?
To understand morning knee stiffness causes and relief, start with cartilage. It has no blood supply of its own. It cannot receive nutrients directly the way muscle or bone does. Instead, it relies entirely on movement to absorb what it needs from the synovial fluid surrounding it. Every step you take compresses the cartilage slightly, squeezes fluid through it, then lets fresh fluid flow back in. That is how the joint feeds itself.
When you stop moving for hours, that exchange stops too. The fluid thickens. The cartilage sits without fresh lubrication. And the joint structures that normally glide smoothly have to work harder to get going again.
This is why rest does not solve morning knee stiffness. It is also why those first two minutes of movement feel so different from the two minutes after that. The joint is not broken. It is warming up.
How long should morning knee stiffness last?
In adults with knee osteoarthritis, morning stiffness that resolves within 30 minutes of movement is a recognized clinical pattern. A JAMA review identified morning stiffness lasting less than 30 minutes as a key diagnostic marker for knee OA, with 95% sensitivity (Duong et al., 2023). Stiffness that eases once you start moving is consistent with what clinicians expect. It is part of the condition, not a sign of deterioration.
What warrants attention is stiffness that persists well beyond 30 minutes most mornings, or stiffness accompanied by swelling, heat, or redness. Those patterns suggest something beyond the typical morning knee stiffness causes and relief cycle and deserve a conversation with your physician.
For most adults over 55, stiffness that loosens within the first 20 to 30 minutes is the body doing exactly what it is supposed to do once movement begins.
What is the one thing that actually helps?
Movement. Specifically, walking.
Not a long walk. Not a workout. Just enough movement to start redistributing the synovial fluid, engage the muscles around the knee, and let the joint warm up the way it is designed to.
Research on exercise and knee osteoarthritis consistently shows that low-impact movement reduces both pain and stiffness, with walking among the most supported approaches for adults in this age group (Fransen et al., 2015). The benefit is not just long-term. It starts within the first few minutes of the first session.
For morning knee stiffness causes and relief, the timing matters as much as the movement itself. Walking within the first few minutes of waking, before you sit back down with coffee or check your phone, gives the joint its best chance to loosen up before the day asks anything harder of it.
Two minutes is enough to start. The joint does not need much. It just needs to move.
What does a 3-minute morning movement routine look like?
A 3-minute morning movement routine for adults over 55 with stiff knees. Three steps. No equipment. Do this every morning before anything else.
Drink a glass of water
Your joints need hydration to produce healthy synovial fluid. A glass of water before you move is a small signal that the day is starting.
Walk for 2 minutes
Easy pace. Around the house, down the hallway. You are not training. You are giving the joint what it needs to redistribute fluid and warm up the cartilage surfaces.
Stop and close your eyes for 30 seconds
Stand still. Breathe. Notice how your knees feel now compared to when you first got up. That shift is the joint responding to movement the way it was designed to.
For morning knee stiffness relief, consistency matters more than duration. Three minutes every morning beats thirty minutes three times a week.
Wrap-up: Why are my knees so stiff in the morning?
Because they have been still for hours, and they need you to move.
Morning knee stiffness causes and relief are two sides of the same mechanism. The joint thickens when it rests and loosens when it moves. That is not a problem to solve. It is a pattern to work with.
What changes outcomes is not finding the perfect stretch or the right supplement. It is showing up for two minutes every morning before the day gets in the way. Consistently. Before coffee. Before your phone. Before anything else asks something of your knees.
Morning stiffness is one piece of the larger picture of knee pain relief for adults over 55. Your body already knows how to do this. It just needs the chance.
Nothing in this post substitutes for a conversation with your physician. If you are uncertain whether your knee pain is safe to work with, start there.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Frequently Asked Questions
Is morning knee stiffness a sign of arthritis?
It can be, but it is not automatically a cause for concern. Morning knee stiffness causes and relief follow a predictable pattern in knee osteoarthritis: the joint stiffens with inactivity and loosens with movement. Stiffness that resolves within 30 minutes is consistent with OA. Stiffness lasting longer, or accompanied by swelling or heat, warrants a physician’s evaluation.
How long should morning knee stiffness last?
For adults with knee osteoarthritis, morning stiffness that eases within 20 to 30 minutes of moving around is a recognized clinical pattern (Duong et al., 2023). Morning knee stiffness lasting beyond 30 minutes is a different pattern than typical morning knee stiffness causes and relief.
What stretches help stiff knees in the morning?
The most effective thing for morning knee stiffness relief is not a stretch. It is walking. Even two minutes of easy movement redistributes synovial fluid and reduces stiffness faster than static stretching. If you want to add gentle range-of-motion work, slow ankle circles and knee bends while still in bed before you stand up are a reasonable addition.
Does morning stiffness get worse with age?
It can become more noticeable as cartilage thins and synovial fluid production changes with age. But morning knee stiffness causes and relief remain the same regardless of age — the joint responds to movement. Adults who walk consistently in the morning report less stiffness over time, not more (Fransen et al., 2015). The habit matters more than the age.
FAQ 5: Can walking really reduce morning knee stiffness?
Yes, and the mechanism is direct. Walking redistributes synovial fluid, compresses and nourishes cartilage, and engages the muscles that support the joint. Research on exercise and knee osteoarthritis consistently shows that low-impact movement reduces both stiffness and pain over time (Fransen et al., 2015). Two minutes first thing in the morning is enough to start that process.
Is it normal for knees to be stiff every morning?
For adults over 55 with knee osteoarthritis, yes. Morning stiffness that resolves within 30 minutes of movement is a recognized clinical pattern, not a sign of something getting worse (Duong et al., 2023). If your stiffness resolves once you start moving, your joint is responding the way it is supposed to. Stiffness that persists beyond 30 minutes most mornings is worth discussing with your physician.
References
Duong, V., Oo, W. M., Ding, C., Culvenor, A. G., & Hunter, D. J. (2023). Evaluation and treatment of knee pain: A review. JAMA, 330(16), 1568–1580. https://doi.org/10.1001/jama.2023.19675
Fransen, M., McConnell, S., Harmer, A. R., Van der Esch, M., Simic, M., & Bennell, K. L. (2015). Exercise for osteoarthritis of the knee: A Cochrane systematic review. British Journal of Sports Medicine, 49(24), 1554–1557. https://doi.org/10.1136/bjsports-2015-095424
One question I hear more than almost any other is this: “Coach D, does walking help knee arthritis, or does it make things worse?”
It is a fair question. When your knees hurt, walking feels like the last thing you should be doing. The instinct is to rest, protect, and wait for something to change.
But here is what the research actually shows about whether walking helps knee arthritis. A study following more than 1,200 adults with knee osteoarthritis found that those who walked for exercise had 40% lower odds of developing frequent knee pain compared to those who did not (Lo et al., 2022). Same diagnosis. Very different outcomes. The difference was whether walking was happening consistently.
If you have been wondering whether walking helps knee pain or makes things worse, the answer is clearer than most people realize.
KEY TAKEAWAY
Yes. Walking for exercise helps with knee pain. Adults with knee osteoarthritis who walk regularly have significantly lower odds of developing frequent knee pain and show less structural joint damage over time compared to those who do not walk (Lo et al., 2022).
Here is what the research shows about how walking protects the knee, how much you need, and what to watch out for as you build the habit.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
Does walking actually help knee arthritis?
The short answer is yes. And the evidence behind that answer is more substantial than most people with knee arthritis have ever been told.
Does walking help knee arthritis? A large observational study of more than 1,200 adults with knee osteoarthritis found that those who walked for exercise had 40% lower odds of developing frequent knee pain compared to those who did not (Lo et al., 2022). The walkers also showed less structural joint damage on X-ray over the follow-up period. Same diagnosis. Less progression. The difference was consistent walking.
What makes this finding particularly meaningful is the population it studied. These were adults aged 50 and older who already had radiographic evidence of osteoarthritis. Not people trying to prevent the condition. People who already had it. And walking still made a measurable difference.
There is also a statistic worth knowing on the other side of this. Only 39% of adults with osteoarthritis receive a referral or recommendation to exercise from their primary care provider (Keogh et al., 2024). That means the majority of people with knee arthritis are never told about the one intervention with the clearest evidence behind it. If nobody told you walking was this effective, that is not an oversight on your part. It is a gap in how osteoarthritis care gets delivered.
How does walking protect your knee joint?
Think of cartilage like a sponge. It has no blood supply of its own. The only way it receives nutrients and stays healthy is through movement. Every step you take compresses the cartilage and squeezes fluid out, then as the weight lifts, fresh nutrient-rich fluid flows back in. Stop moving, and the cartilage starts to starve.
That is why walking to help knee arthritis is a better question than most people think to ask. Joints are not like car tires grinding down with use. They are living tissue that depends on movement for repair. The research describes it more accurately as a process of wear and repair, and walking tips that balance in your favor.
Walking also strengthens the muscles that surround your knee. Those muscles, particularly the quadriceps, are your joints’ primary shock absorbers. When they are strong, they take on the load that would otherwise fall directly on the cartilage and bone. Research on aerobic walking for knee osteoarthritis consistently shows that this muscle-building effect reduces both pain and functional limitation over time (Roddy et al., 2005).
There is one more thing worth knowing. Fewer than 4 in 10 adults with osteoarthritis are ever referred to exercise by their primary care provider (Keogh et al., 2024). Most people who wonder whether walking helps knee arthritis never get a clear answer from the people treating them. The research has been available for decades. It just has not been making its way into the room where it matters most.
What does the research actually show?
The research on walking and knee osteoarthritis is more consistent than most people realize. A large observational study following more than 1,200 adults aged 50 and older with knee osteoarthritis found that those who walked for exercise had 40% lower odds of developing frequent knee pain compared to those who did not walk (Lo et al., 2022). That is a substantial difference for an activity that requires no equipment, no gym, and no prescription.
The same study found that walkers also showed less structural joint damage on X-ray over the follow-up period. That matters because it suggests walking does not just help people feel better. It may slow the physical progression of the condition itself.
The Cochrane review of exercise and knee osteoarthritis, which pooled data from dozens of randomized controlled trials, confirms the same direction. Exercise reduces pain and improves function in adults with knee osteoarthritis, with low-impact aerobic activity like walking among the most consistently supported approaches (Fransen et al., 2015).
What the research does not support is the idea that walking with arthritis damages the joint further. For most adults with mild to moderate knee osteoarthritis, the evidence consistently points the other way. The joint does not wear out faster with use. Used correctly, it responds.
This is where most advice about whether walking helps knee arthritis goes wrong. It jumps straight to targets like 10,000 steps or 30 minutes a day without accounting for where you are starting from. For adults with knee arthritis, the starting point matters more than the target.
The research on how much walking helps knee arthritis points to consistency over volume. The Lo et al. (2022) study classified participants as walkers if they reported 10 or more instances of walking for exercise since age 50. That is not a daily target. It is a pattern. Adults who walked regularly, even if not every day or for long durations, experienced meaningfully better outcomes than those who did not walk at all.
A practical framework based on the evidence looks like this:
Start shorter than feels necessary. Five to ten minutes is a real session. It is enough to compress and nourish the cartilage, engage the supporting muscles, and establish the habit.
Build gradually. Add one to two minutes per session every few days when your knees are responding well. The signal that guides you is how your knees feel in the two to four hours after a walk, not during it.
Aim for consistency over distance. Three to five sessions per week of walking can sustain matters more than occasional long walks that leave your knees paying for it the next day.
There is no single number that works for every person with knee arthritis. Your body’s response is the most reliable guide you have.
What should you watch out for when walking with arthritis?
Does walking help knee arthritis when it already hurts? For most adults with mild to moderate osteoarthritis, yes. But there are a few things worth knowing before you start, because how you walk matters as much as whether you walk.
Pain during the walk versus pain after. Some discomfort during a walk is normal, particularly in the early weeks. The signal that matters is what happens two to four hours afterward. If your knees feel meaningfully worse in that window, the session was longer or more intense than your joint was ready for. Shorten the next session rather than stopping altogether.
Sharp pain, swelling, or instability are different. These are not the normal discomfort of a joint being asked to work. They are signals to stop and check in with your physician before continuing. Walking through this kind of pain does not build tolerance. It adds load to a joint that is telling you something important.
Footwear matters more than most people expect. Cushioned, supportive sneakers with a firm midsole reduce the impact your knees absorb with each step. Worn-out soles that have compressed visibly are no longer doing that job. If your walking shoes are more than a year old and you walk regularly, they have likely passed their useful life for joint protection.
Surface and pace work together. Softer surfaces reduce impact. A conversational pace keeps the load manageable. Neither factor matters as much as session length in the early weeks, but both help when you are trying to find a rhythm that your knees respond well to.
Nothing in this section replaces a conversation with your physician, particularly if you are managing a specific diagnosis, recent surgery, or significant swelling.
Wrap-up: Does walking help knee arthritis?
Yes. And the evidence behind that answer is more substantial than most adults with knee arthritis have ever been told.
Walking for exercise reduces the odds of developing frequent knee pain by 40% in adults with osteoarthritis (Lo et al., 2022). It nourishes cartilage that has no other way to receive nutrients. It strengthens the muscles that protect the joint from the load it was never meant to absorb alone. And it does this without equipment, without a gym, and without pushing through pain that signals something is wrong.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Frequently Asked Questions
Does walking help knee arthritis or make it worse?
The short answer to whether walking helps knee arthritis is yes, and the evidence is specific. A study of more than 1,200 adults with knee osteoarthritis found that those who walked for exercise had 40% lower odds of developing frequent knee pain compared to those who did not walk (Lo et al., 2022). The same study found that walkers showed less structural joint damage over time. Walking does not wear the joint out faster. Used consistently and at the right level, it supports the repair process that the joint depends on.
How much walking is good for knee arthritis?
Consistency matters more than duration, especially at the start. Begin with five to ten minutes at a comfortable pace and build gradually based on how your knees respond in the two to four hours after each session. Three to five sessions per week is a reasonable target. The research supports accumulated walking over time, not daily distance goals.
Is it okay to walk when my knees hurt from arthritis?
Mild discomfort during a walk is normal and does not mean you are causing damage. The signal to pay attention to is how your knees feel two to four hours afterward. Sharp pain, swelling, or instability during a walk are different and warrant a conversation with your physician before continuing. If you are uncertain whether walking is appropriate for your specific situation, start there.
What type of walking is best for knee arthritis?
Flat surfaces, a conversational pace, and supportive footwear create the conditions where walking is most likely to help knee arthritis without adding unnecessary load to the joint. Shorter sessions done consistently outperform occasional long walks. The goal in the early weeks is to find a pattern your knees respond well to, then build from there.
How long does it take for walking to help knee arthritis?
The Lo et al. (2022) study tracked participants over 48 months and found meaningful differences between walkers and non-walkers in both pain and structural outcomes. In practice, most adults notice that their knees stop paying for their walks in the days or weeks after starting a consistent pattern, before they notice any reduction in baseline discomfort. Consistency over weeks and months is what produces lasting change.
Is cycling or swimming better than walking for knee arthritis?
Does walking help knee arthritis more than cycling or swimming? The evidence base for walking is strong and specific. The research base for walking and knee osteoarthritis is strong and specific (Lo et al., 2022; Fransen et al., 2015). Walking also builds the functional capability most adults with knee arthritis actually want back. If walking is accessible and your knees tolerate it, it is worth prioritizing.
References
Fransen, M., McConnell, S., Harmer, A. R., Van der Esch, M., Simic, M., & Bennell, K. L. (2015). Exercise for osteoarthritis of the knee: A Cochrane systematic review. British Journal of Sports Medicine, 49(24), 1554–1557. https://doi.org/10.1136/bjsports-2015-095424
Keogh, A., Toomey, C., Matthews, J., & Hurley, D. A. (2024). Guideline-based exercise management for hip and knee osteoarthritis: a cross-sectional comparison of healthcare professional and patient beliefs in Ireland. BMJ Open, 14(1), e079019. https://doi.org/10.1136/bmjopen-2023-079019
Lo, G. H., Vinod, S., Richard, M. J., Harkey, M. S., McAlindon, T. E., Kriska, A. M., Rockette-Wagner, B., Eaton, C. B., Hochberg, M. C., Jackson, R. D., Kwoh, C. K., Nevitt, M. C., & Driban, J. B. (2022). Association between walking for exercise and symptomatic and structural progression in individuals with knee osteoarthritis: Data from the Osteoarthritis Initiative Cohort. Arthritis & Rheumatology, 74(10), 1660–1667. https://doi.org/10.1002/art.42241
Roddy, E., Zhang, W., & Doherty, M. (2005). Aerobic walking or strengthening exercise for osteoarthritis of the knee: A systematic review. Annals of the Rheumatic Diseases, 64(4), 544–548. https://doi.org/10.1136/ard.2004.028746
I have watched people manage knee pain for years. The ones who struggle most are rarely the ones with the most severe physical symptoms. They are the ones carrying something nobody ever addressed: the emotional weight that builds up quietly alongside the pain.
Nobody told them that chronic knee pain has a documented psychological dimension. Nobody mentioned that the frustration, the low motivation, the creeping sense of isolation. Those are not character flaws. They are recognized patterns that show up in the research consistently.
If the emotional impact of chronic knee pain has been affecting you more than you let on, you are not alone, and you are not overreacting. This post addresses the part that most knee pain programs completely skip.
Key Takeaway
Research analyzing 49 studies and 15,855 individuals found that one in five adults with osteoarthritis experience symptoms of depression, and a similar proportion experience anxiety (Stubbs et al., 2016). The emotional side of chronic knee pain is not incidental. It is part of the condition.
Here is what the research shows about how chronic knee pain affects mood, identity, and self-perception, and what a whole-person approach actually does about it.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
Does chronic knee pain actually cause depression?
The emotional side of chronic knee pain and depression are more closely linked than most people realize. Research analyzing 49 studies and more than 15,000 individuals found that one in five adults with osteoarthritis experience symptoms of depression, with a similar proportion reporting anxiety (Stubbs et al., 2016). The emotional effects of chronic knee pain are not a side issue. They are part of the clinical picture.
That does not mean knee pain causes depression in every person who has it. What the research shows is that the rate is significantly elevated compared to the general population. Living with persistent pain changes things. It limits what you can do. It interrupts sleep. It shifts the way you think about your body and your future. Those are not small things, and their cumulative effect on mood is real and measurable.
What matters for you is recognizing that if you have been feeling lower than usual since your knee pain started, that pattern has a name. It is not a weakness. It is not a lack of gratitude. It is a documented response to living with a chronic physical condition that most people manage in silence.
The first step toward addressing it is naming it honestly, which is what the rest of this post does.
Why does knee pain affect your mood and motivation?
Chronic pain and anxiety often travel together, and the reason comes down to what pain quietly removes from your life. It is not just the physical limitation. It is everything that physical limitation takes with it.
When knee pain makes walking uncomfortable, you stop going to the places that walking took you. The morning walks with a neighbor. The errands you ran yourself. The grandchildren you kept up with. As those things disappear, so do the social connections, the sense of capability, and the daily rhythm that kept your mood regulated. The absence is gradual enough that most people do not notice it happening until they look back and realize how much has changed.
Research on cognitive and behavioral factors in knee pain found that how you think about your pain directly shapes how much it affects your life (Urquhart et al., 2015). Adults who developed a strong sense that their body could still do things reported significantly better function and mood outcomes than those who did not. Adults who began to fear movement, anticipating that any activity would make things worse, experienced higher pain levels and greater limitation over time.
This is not about positive thinking as a cure. It is about recognizing that knee pain and mental health are connected in both directions. Pain affects mood. Mood affects how much pain you experience and how well you function. Breaking into that cycle is part of what recovery actually requires.
The first place that the cycle can be interrupted is in how you understand what is happening to you. Not just in the joint. In the whole experience of living with it.
What does chronic knee pain do to your sense of identity?
This is the part of the emotional side of chronic knee pain that nobody talks about. Chronic pain and social isolation are well-documented together, but the deeper loss is harder to name. It is not just that you see fewer people. It is that the activities that told you who you were have quietly stepped back, one by one.
Maybe you were the person who walked every morning. The grandparent who got down on the floor. The one in your group who suggested the hike, organized the trip, and kept up with everyone else. Knee pain did not just make those things harder. It began to rewrite the story you told yourself about what kind of person you are.
That shift in identity is real, and it compounds. When knee pain limits your quality of life long enough, many adults begin to define themselves by what they can no longer do rather than what they still can. The activities that once gave them energy, confidence, and connection start to feel like reminders of loss instead of possibilities. Motivation drops not because of laziness but because the future feels smaller than it used to.
What is worth knowing is that this pattern is recognized, and it is not permanent. The research on cognitive factors and knee pain is clear that identity and self-belief are modifiable (Urquhart et al., 2015). Adults who rebuild a sense of what their body is capable of, even starting from very small wins, show measurably better outcomes than those who do not.
You are not the sum of what your knees currently prevent. That story is still being written.
How does the way you talk to yourself affect your knee pain?
Mindset and chronic pain are connected in ways that go beyond attitude. The research on cognitive factors in knee pain found that adults with high pain self-efficacy, a belief that their body was still capable, reported significantly better function and lower pain levels than those without it (Urquhart et al., 2015). How you think about your body is not separate from how your body performs. It is part of the same system.
This shows up in a specific way with knee pain. When pain has been present long enough, many adults develop a habit of bracing for it. They anticipate the worst before each walk. They interpret every twinge as confirmation that things are getting worse. That pattern of thinking amplifies how pain feels and makes movement feel more threatening than it is. The result is less movement, more stiffness, and a stronger belief that the body cannot be trusted. The cycle reinforces itself.
The way you talk to yourself about your body either opens that cycle or closes it. Small, honest encouragement works differently from false positivity. It is not about telling yourself the pain is not there. It is about noticing when your body does something it could not do last week, however small, and letting that register.
That kind of internal language is something you can practice. It does not require a program or a framework. It starts with paying attention to what you say to yourself in the two minutes after a walk, and choosing something accurate and encouraging instead of defaulting to what still hurts.
What does a whole-person approach to knee pain actually look like?
Holistic knee pain management is a phrase that gets used loosely, but what it means in practice is straightforward. It means treating the physical, nutritional, and emotional dimensions of knee pain at the same time, not one after the other.
Most knee pain programs address the joint. Some address movement. Very few address what is happening in the mind and the identity of the person living with the pain. That gap is not a minor oversight. Research consistently shows that exercise reduces pain and improves function in adults with knee osteoarthritis (Fransen et al., 2015), but adherence, actually doing the movement consistently, depends heavily on whether the emotional and psychological side is being addressed alongside it.
A mind-body approach to knee pain looks like this in practice:
Meals that reduce the inflammatory baseline your joints are working against every day, so that movement feels more possible and recovery happens faster.
Mindfulness that addresses the thought patterns, the self-talk, and the emotional weight that chronic pain accumulates over time.
None of these three works as well alone as all three do together. Managing knee pain naturally means managing the whole experience of having it, not just the tissue.
That is what the research points toward. It is also what most adults with chronic knee pain have never been offered.
Wrap-up: the emotional side of chronic knee pain
Chronic knee pain is not just a joint problem. The research is clear on this. One in five adults with osteoarthritis experiences depressive symptoms. A similar proportion experience anxiety. The isolation, the identity shift, the quiet erosion of motivation, these are not personal failures. They are documented patterns that show up consistently when pain is present long enough and goes unaddressed as a whole experience.
The physical side of knee pain gets most of the attention. The emotional side of chronic knee pain gets almost none. That imbalance is part of why so many adults manage their symptoms for years without making meaningful progress. They are working on one part of a three-part problem.
What changes outcomes is addressing all three parts together. Movement that builds slowly and builds confidence alongside capability. Food choices that lower the inflammatory baseline the joint is working against. And honest attention to the mental and emotional load that chronic pain carries with it, including how you talk to yourself about what your body can do.
You do not have to have everything figured out before you start. The smallest possible starting point is still a starting point. The 3-Minute Knee Test is exactly that, a structured way to find out what your body responds to, before you commit to anything more.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Frequently Asked Questions
Can chronic pain cause depression?
Yes. Research analyzing 49 studies and more than 15,000 adults with osteoarthritis found that one in five experience symptoms of depression, with a similar proportion reporting anxiety (Stubbs et al., 2016). The emotional side of chronic knee pain includes documented impacts on sleep, mood, and daily motivation. The emotional effects of chronic knee pain are not incidental. They are a recognized and documented part of living with persistent pain.
Why does knee pain make me feel isolated?
Because knee pain limits the activities that connect you to other people. Walking with friends, keeping up with grandchildren, attending events that require being on your feet, when those things become difficult, the social fabric that supported your mood and sense of belonging quietly thins. That is not a weakness. It is a predictable consequence of chronic pain and social isolation that researchers have documented consistently.
How does mindset affect knee pain recovery?
Research on cognitive factors in knee pain found that adults with a strong belief in their body’s capability reported significantly better function and lower pain levels than those without it (Urquhart et al., 2015). Mindset and chronic pain are connected in both directions. How you think about your body affects how much you move. How much you move affects how your body feels. Building a realistic, encouraging internal narrative about small progress is part of what recovery actually requires.
Is it normal to feel anxious about your knee pain getting worse?
Very common, yes. Fear of movement is one of the most documented cognitive patterns in chronic knee pain. Many adults begin to anticipate pain before it arrives, which leads them to move less, which leads to more stiffness and greater limitation over time. Recognizing that pattern is the first step toward changing it. If anxiety about your knees is affecting your daily decisions, that is worth addressing directly alongside the physical side of your pain.
What does a whole-person approach to knee pain look like?
It means addressing movement, nutrition, and the emotional and mental dimensions of knee pain at the same time rather than one after the other. Exercise reduces pain and improves function in adults with knee osteoarthritis (Fransen et al., 2015), but sustained progress depends on whether the psychological side is being addressed alongside it. A whole-person approach combines movement that builds confidence, food choices that reduce inflammation, and attention to the thought patterns that chronic pain creates over time.
Can improving your mood actually reduce knee pain?
The relationship runs in both directions. Pain affects mood, and mood affects pain perception. Research on cognitive factors in knee pain found that how you think about your body — your level of self-belief, your expectations about what is possible — directly influences your functional outcomes (Urquhart et al., 2015). Addressing the emotional side of chronic knee pain is not a soft add-on to physical treatment. It is part of what determines how well the physical treatment works.
References
Fransen, M., McConnell, S., Harmer, A. R., Van der Esch, M., Simic, M., & Bennell, K. L. (2015). Exercise for osteoarthritis of the knee: A Cochrane systematic review. British Journal of Sports Medicine, 49(24), 1554–1557. https://doi.org/10.1136/bjsports-2015-095424
Stubbs, B., Aluko, Y., Myint, P. K., & Smith, T. O. (2016). Prevalence of depressive symptoms and anxiety in osteoarthritis: a systematic review and meta-analysis. Age and Ageing, 45(2), 228–235. https://doi.org/10.1093/ageing/afw001
Urquhart, D. M., Phyomaung, P. P., Dubowitz, J., Fernando, S., Wluka, A. E., Raajmaakers, P., Wang, Y., & Cicuttini, F. M. (2015). Are cognitive and behavioural factors associated with knee pain? A systematic review. Seminars in Arthritis and Rheumatism, 44(4), 445–455. https://doi.org/10.1016/j.semarthrit.2014.07.005
I used to think longer walks meant better results. More time on your feet, more benefit for your knees. It seemed logical. It was wrong.
What the research actually shows surprised me when I first came across it. A study comparing continuous walking with shorter bouts in adults with knee osteoarthritis found that continuous walking increased knee pain over time, while the shorter bouts did not (Farrokhi et al., 2017). Same total walking time. Very different experience for the knees.
If you have been searching for a short-burst walking approach that works for knee pain after 55, the research behind it is more specific than most people realize.
For adults who have been cutting their walks short because their knees start complaining after ten or fifteen minutes, that instinct may be exactly right. You are not failing at walking. You may be doing precisely what your knees need without knowing it.
Key Takeaways
For adults with knee osteoarthritis, shorter bouts of walking outperform one long continuous session for managing knee pain during exercise. Research comparing the two found that continuous walking increased knee pain while interval walking did not, even when total walking time was equal (Farrokhi et al., 2017).
Here is what the research shows about why short bursts work better, how to structure them, and what to pay attention to as you build your walking habit.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
Why does walking start to hurt after a certain point?
If your knees feel reasonable at the start of a walk and progressively worse as you keep going, that is not just how things are. There is a mechanical reason for it.
When you walk continuously for an extended period, the muscles surrounding your knee gradually fatigue (Doherty, 2003). Those muscles, particularly the quadriceps, are your knee’s primary shock absorbers. When they are fresh, they absorb a meaningful portion of the force each step produces. As they tire, they absorb less of it. The joint itself takes on more of that load with every subsequent step.
Research measuring knee contact forces during walking found that forces increased significantly after 30 minutes of continuous walking in adults with knee osteoarthritis, regardless of pace (Farrokhi et al., 2017). The joint was absorbing more load at 30 minutes than it was at minute one. That increased loading corresponded directly with increased knee pain in the continuous walking group.
This matters because most generic walking advice assumes the goal is to build toward longer and longer sessions. For adults over 55 with knee concerns, that assumption skips a critical variable. Duration is not neutral. After a certain point, it starts working against you.
The good news is that the same study found a straightforward way around this. You do not have to walk less. You have to walk differently.
What does the research say about shorter walking bouts and knee pain?
The evidence here is more specific than most people realize. It is not just that shorter walks feel better. There is a measurable mechanical reason why they are better.
Farrokhi et al. (2017) compared two groups of adults with knee osteoarthritis. One group walked continuously for 45 minutes. The other group walked in three separate 15-minute bouts with rest periods in between — the same total walking time, broken up. The findings were clear:
Continuous walking increased knee pain over time. The interval walking group experienced no significant increase in knee pain, even though they walked the same total distance.
The researchers also measured knee contact forces throughout both sessions. After 30 minutes of continuous walking, joint loading increased by 22 to 25 percent above baseline. That is the joint absorbing significantly more force than it was at the start, because the surrounding muscles had fatigued and stopped doing their share of the work.
The interval group did not escape the loading increase entirely. But they did escape the pain increase. The rest periods between bouts allowed the muscles to partially recover before the next session began. The joint never reached the sustained loading threshold that the continuous walkers hit.
For adults over 55 with knee concerns, this finding reframes the whole question. The goal is not to build toward a 30-minute continuous walk as fast as possible. The goal is to accumulate walking time in a way that keeps your knees responding well throughout. That is a different target, and it changes how you start.
How do you structure short walking bouts when your knees are sore?
The research used 15-minute bouts with one-hour rest periods. That is the clinical format. For most adults starting out with knee concerns, that structure is actually more than you need to begin with.
Here is a practical starting framework:
Start at 5 to 10 minutes per bout. Not 15. If your knees have been limiting your walking for weeks or months, start shorter than feels necessary. You can always add time. You cannot undo a session that pushed too far.
Rest between bouts means actual rest. Sitting or light activity. Not another form of exercise. The muscles surrounding your knee need enough recovery time to be useful again before the next walk.
Two to three bouts per day is a reasonable starting target. Morning, midday, and late afternoon work well for many adults. The specific times matter less than the consistency.
Track how your knees feel two to four hours after each bout, not during it. Post-session feedback is your most reliable data point. Discomfort that ramps up hours later means shortening the next bout. Discomfort that stays flat or fades means you are working at the right level.
One thing to be clear about. This is not a permanent structure. It is a starting point. As your joint tolerance builds and your supporting muscles get stronger, the bouts get longer and the rest periods get shorter. That progression happens on your body’s timeline, not a generic program’s.
How do you know if short bursts are working for you?
The most common mistake adults make when starting any new movement approach is measuring the wrong thing. They check how their knees feel during the walk. That is useful information, but it is not the number that tells you whether the approach is working.
The two to four-hour window after a bout is your real data point.
Here is a simple tracking framework:
What to track
What it tells you
Pain during the bout
Whether the current session length is too long
Pain 2 to 4 hours after
Whether the overall load was appropriate
Pain the following morning
Whether cumulative load is building correctly
Energy and mood after
Whether the approach is sustainable
If your knees feel roughly the same or better two to four hours after a bout, you are working at the right level. If they feel meaningfully worse, shorten the next bout before you add anything else.
Progress with this approach is not always linear and it is rarely dramatic in the first week. What most adults notice first is not a reduction in knee pain during walks. It is that the pain after walks stops escalating. The walks stop costing them the rest of the day. That is the first signal that the approach is working.
From there, the bouts get longer. The rest periods get shorter. The daily total accumulates. The pattern builds on itself when the foundation is right.
What else affects how your knees respond during a walk?
The approach of breaking walking into shorter sessions with rest in between is the most important variable. But several other factors influence how your knees respond, and getting them right makes the difference between a session that builds your capacity and one that just adds to the load.
Surface. Packed dirt, grass, or a rubberized track absorbs more impact than concrete or asphalt. If you have a choice, use the softer surface. If you do not, the session length matters more than the surface. A 5-minute walk on concrete is still better than a 30-minute walk on a trail.
Footwear. Cushioned, supportive sneakers with a firm midsole reduce the impact your knees absorb with each step. Worn-out soles that have compressed visibly are no longer doing that job. If your walking shoes are more than a year old and you walk regularly, they are likely past their useful life for joint protection.
Pace. Comfortable and conversational is the right pace for short walks. You should be able to speak a short sentence without effort. Moving faster than that during the early weeks adds load without adding benefit. Speed becomes relevant later, once your joint tolerance has built and the pattern of shorter sessions is well established.
Time of day. Many adults with knee concerns find that morning walks feel stiffer than afternoon walks. A few minutes of light movement before your first walk redistributes that stiffness and makes the first session feel considerably different.
None of these factors replaces the foundation. Think of them as variables you can adjust once you have the habit of short, broken-up walking sessions in place.
Wrap-up: why short bursts of walking work better for sore knees after 55
The instinct when your knees hurt during a walk is to push through or stop entirely. The research points to a third option that most adults over 55 have never been given: walk shorter, more often, with rest in between.
Farrokhi et al. (2017) found that continuous walking increased knee pain in adults with osteoarthritis while interval walking did not, even when the total walking time was identical. The difference was not effort or willpower. It was structure. Shorter sessions keep the muscles around your knee functional throughout the walk. They never reach the fatigue threshold where the joint starts absorbing load on its own.
That one shift changes what walking feels like after 55. Not easier in the sense of requiring less from you. Easier in the sense that your knees stop making you pay for it afterward.
Start with sessions your knees can handle. Track how you feel two to four hours later. Build from there. The 3-Minute Knee Test is the smallest possible starting point — a structured way to find out what your body responds to before you commit to anything more.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Frequently Asked Questions
Is it better to walk for 10 minutes three times a day or 30 minutes all at once for knee pain?
For adults over 55 with knee concerns, three shorter sessions outperform one long continuous walk. Research found that continuous walking increased knee pain in adults with osteoarthritis, while the same total walking time broken into shorter bouts did not (Farrokhi et al., 2017). The muscles surrounding your knee stay more functional throughout shorter sessions, which means the joint absorbs less unassisted load.
How long should I rest between short walking sessions?
The research used one-hour rest periods between 15-minute bouts. For most adults starting out, that is a reasonable guideline. The goal of the rest period is to allow the muscles surrounding your knee to partially recover before the next session. If you find that one hour is not enough and your knees feel worse going into the second bout, extend the rest. Your post-session feedback is more reliable than any fixed number.
Can I do other activities between my short walking sessions?
Light activity is fine. Sitting, gentle stretching, or everyday household movement between sessions will not undermine the rest period. What you want to avoid is stacking another form of loading exercise directly before or after a walking session. The goal is to let the muscles around your knee recover enough to be useful for the next walk.
What if my knees feel fine during the walk but hurt later?
That is your most important signal. Discomfort that surfaces two to four hours after a session means the session was longer or more intense than your joint was ready for. Shorten the next session rather than stopping altogether. The pattern you are looking for is walks that leave your knees feeling roughly the same or better in that two-to-four-hour window, not worse.
How do I know when I am ready to make my walking sessions longer?
When your knees consistently feel the same or better in the two to four hours after a session, and that pattern holds for at least five to seven consecutive days, you are ready to add one to two minutes to each session. Do not increase more than one variable at a time. Add duration first. Add frequency later. Add pace last.
Does walking in short sessions build the same fitness as one long walk?
For adults managing knee pain, the priority at the start is joint tolerance, not cardiovascular fitness. Short sessions done consistently do build aerobic capacity over time, and research supports accumulated walking time as an effective approach for overall health outcomes. The difference is that shorter sessions allow you to accumulate that time without the joint loading that comes with continuous walking past the 30-minute mark. As your capacity builds and your sessions get longer, the fitness benefits compound alongside the joint benefits.
Farrokhi, S., Jayabalan, P., Gustafson, J. A., Klatt, B. A., Sowa, G. A., & Piva, S. R. (2017). The influence of continuous versus interval walking exercise on knee joint loading and pain in patients with knee osteoarthritis. Gait & Posture, 56, 129–133. https://doi.org/10.1016/j.gaitpost.2017.05.024
Fransen, M., McConnell, S., Harmer, A. R., Van der Esch, M., Simic, M., & Bennell, K. L. (2015). Exercise for osteoarthritis of the knee: A Cochrane systematic review. British Journal of Sports Medicine, 49(24), 1554–1557. https://doi.org/10.1136/bjsports-2015-095424
Roddy, E., Zhang, W., & Doherty, M. (2005). Aerobic walking or strengthening exercise for osteoarthritis of the knee: A systematic review. Annals of the Rheumatic Diseases, 64(4), 544–548. https://doi.org/10.1136/ard.2004.028746
Knee pain relief for adults over 55 comes down to three factors working together: how you move, what you eat, and how you think about your body. Rest alone does not change the pattern. A Cochrane review of 54 trials found that exercise consistently improves function and reduces discomfort in adults with knee osteoarthritis (Fransen et al., 2015). This guide covers all three factors and links to the research behind each one.
I spent years telling people that knee pain was something you managed, not something you changed. That was wrong. Not because I was trying to mislead anyone. Because nobody had shown me the full picture yet.
The research on knee pain and adults over 55 is clearer than I expected. Movement done correctly does not make knee pain worse. What you eat affects how your joints feel every single day. And the way I think about my own knees, what I believed was possible after three surgeries, turned out to matter more than I ever would have guessed.
None of those three factors works as well alone as all three do together. That is the idea behind everything on this page.
The three factors that determine outcomes
Most adults who find me have already tried to fix this. They pushed through the pain and paid for it the next day. They followed a walking program or a YouTube routine and ended up worse off than when they started. After a few rounds of that, stopping movement feels like the safe choice.
It is not wrong to stop something that is hurting you. What was missing was not effort. It was a starting point that matched where they actually were, not where a generic program assumed they would be.
Here is what the research points to when all three factors are addressed together.
Movement is the factor most adults get backwards. The instinct when something hurts is to move less. For chronic knee pain in adults over 55, the opposite is true. Joints need movement to stay lubricated. The muscles around your knee need regular load to stay capable of absorbing the force each step produces (Doherty, 2003). A Cochrane review of 54 trials confirmed that exercise consistently improves function and reduces discomfort in adults with knee osteoarthritis (Fransen et al., 2015). The key is not how much you move. It is how you start.
Meals affect the inflammatory environment your joints are operating in every single day. Chronic joint discomfort has an inflammatory component. Foods that drive systemic inflammation raise your baseline before you take a single step. Foods that lower it, fatty fish, leafy greens, olive oil, and berries, work in the other direction over weeks and months of consistent choices. No food reverses structural joint changes. But the environment your joints are working in matters more than most people expect.
Mindfulness is the factor that gets dismissed most often. What you believe about your body shapes what you attempt. What you tell yourself during a difficult walk shapes whether you go again tomorrow. The behavioral side of chronic knee pain is real, measurable, and addressable. It does not fix the joint. It determines whether everything else you do actually sticks.
None of those three factors works as well alone as all three do together. That is what M3 is built on.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
What does a 90-day path to walking 30 minutes actually look like?
What does a 90-day path to walking 30 minutes actually look like?
Most programs hand you a schedule and assume you are starting from a reasonable baseline. A 20-minute walk three times a week. A set of exercises you do in the morning. For adults over 55 who have been avoiding movement because it hurts, that is not a starting point. That is week six of someone else’s program.
A realistic 90-day path starts where you actually are.
The first month is about one thing: showing your body that movement is safe. Sessions are short, often two to three minutes. The goal is not fitness. It is not progress in the traditional sense. It is proof. Proof that you can move without paying for it the next day. That proof is what makes everything after it possible.
The second month builds on that foundation. Sessions get longer. Consistency becomes the focus. You are not just moving. You are building a pattern your body recognizes and expects. That shift from occasional effort to daily habit is where most programs fail people. It is also where the research is clearest about what works.
The third month is when the goal becomes real. Thirty minutes of brisk walking, done comfortably, without cutting it short. Not because you pushed through. Because you built toward it correctly from the beginning.
Nothing in this post substitutes for a conversation with your physician. If you are uncertain whether your knee pain is safe to work with, start there.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Walking and knee pain
Walking and knee pain
These posts cover the research on walking safely with knee pain, why movement helps rather than hurts, and how to build a walking habit that sticks.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Wrap-up: knee pain relief for adults over 55
Knee pain after 55 is not a verdict. It is a pattern. And patterns respond to the right approach applied consistently over time.
Everything on this page points in the same direction. Move correctly. Eat in a way that lowers your baseline inflammation. Address the mental side of living with chronic joint concerns. None of those three works as well alone as all three do together.
The posts in each section above go deeper into every piece of this. Start wherever the question is most urgent for you right now. The 3-Minute Knee Test is the place to begin if you are not sure where that is.
Fransen, M., McConnell, S., Harmer, A. R., Van der Esch, M., Simic, M., & Bennell, K. L. (2015). Exercise for osteoarthritis of the knee: A Cochrane systematic review. British Journal of Sports Medicine, 49(24), 1554–1557. https://doi.org/10.1136/bjsports-2015-095424
Calder, P. C. (2013). Omega-3 polyunsaturated fatty acids and inflammatory processes: Nutrition or pharmacology? British Journal of Clinical Pharmacology, 75(3), 645–662. https://doi.org/10.1111/j.1365-2125.2012.04374.x
Urquhart, D. M., Phyomaung, P. P., Dubowitz, J., Fernando, S., Wluka, A. E., Raajmaakers, P., Wang, Y., & Cicuttini, F. M. (2015). Are cognitive and behavioural factors associated with knee pain? A systematic review. Seminars in Arthritis and Rheumatism, 44(4), 445–455. https://doi.org/10.1016/j.semarthrit.2014.07.005
I did not change what I ate until after my second surgery. Nobody told me to. The focus was always on the joint itself — what to do with it, how to move it, when to rest it. Food felt like a separate conversation.
It is not a separate conversation. It never was.
If you have been looking for the best anti-inflammatory foods for knee pain, here is what I wish someone had told me twenty years ago. What you eat affects the level of inflammation your body is running at baseline. And that baseline is what your knees are working against every time you take a step. Lower the baseline, and the same walk feels different. Not because the joint changed overnight, but because the environment it is operating in did.
KEY TAKEAWAY
Certain foods consistently lower systemic inflammation, which affects how joints feel and function in adults with knee concerns. Omega-3 fatty acids have the strongest research support, with evidence showing they modulate the production of inflammatory compounds at the cellular level (Calder, 2013). No food reverses structural joint changes. But lowering baseline inflammation changes the daily experience of living in a body with knee pain.
Here are seven foods the research points to consistently, what each one actually does, and how to add them without turning your kitchen upside down.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
What do anti-inflammatory foods actually do for your knees?
Before we get to the list, it helps to understand what you are actually trying to accomplish.
Chronic joint discomfort has an inflammatory component. Your body produces inflammatory compounds called cytokines that sensitize joint tissue. When that process is running at a high baseline, your knees start every walk already more irritated than they need to be. The joint is not just dealing with the mechanical load of movement. It is dealing with that load on top of tissue that is already primed to hurt.
Anti-inflammatory foods work by reducing the production of those compounds. Omega-3 fatty acids in particular modulate the body’s inflammatory response at the cellular level, affecting the same pathways that drive chronic joint discomfort (Calder, 2013). The effect is not dramatic or immediate. It is cumulative. Consistent intake over weeks and months shifts the baseline in a direction that makes daily movement more manageable.
What these foods do not do is reverse structural changes in the joint. Cartilage loss, bone spurs, changes that show up on imaging — food choices do not undo those. What they do is change the inflammatory environment those structures are sitting in. That distinction matters because it sets realistic expectations while still making a real case for why this is worth paying attention to.
If you want to understand more about what is driving your knee pain in the first place, I covered the three most common causes of why your knees hurt when you walk. The inflammatory component is one of them, and what you eat connects directly to it.
Why is fatty fish one of the best foods for knee pain?
Fatty fish sits at the top of this list for a reason. Salmon, mackerel, sardines, and herring are the most concentrated dietary sources of EPA and DHA, the two omega-3 fatty acids with the strongest evidence for reducing inflammation.
Here is what they actually do. EPA and DHA modulate the production of inflammatory eicosanoids and cytokines, the compounds your body produces when chronic inflammation is running (Calder, 2013). They do not switch inflammation off. They turn down the volume on a process that, in adults with chronic joint concerns, has been running too loud for too long.
The research on omega-3s and joint health is among the most consistent in the nutritional science space. Most studies use two to three servings of fatty fish per week as the intake level that produces measurable effects on inflammatory markers. That is the context for what the research looks at, not a prescription for what you must eat.
Sardines are worth a special mention here. They are the most affordable option on the list, they are shelf-stable, and they are one of the few foods where you eat the small bones, which adds a meaningful calcium contribution alongside the omega-3s. A can of sardines on whole-grain crackers is not glamorous. It is practical, and it works.
If you do not eat fish, plant-based omega-3 sources exist, and we will get to them. They are a useful addition, but they work differently, and the conversion rate to EPA and DHA is limited compared to direct consumption of fatty fish.
What makes leafy greens worth eating when your knees hurt?
Spinach, kale, Swiss chard, arugula. These are not on this list because they are generally healthy. They are on it because of specific compounds that show up consistently in joint health research.
Leafy greens are high in vitamin K and in antioxidants, including quercetin and kaempferol. Vitamin K plays a role in cartilage metabolism and has been associated with lower rates of knee osteoarthritis progression in observational studies. Quercetin and kaempferol inhibit inflammatory pathways, including some of the same ones targeted by the omega-3s in fatty fish. Different mechanism, same general direction.
The antioxidant piece matters for a reason that often gets overlooked. Chronic inflammation generates oxidative stress, a kind of cellular wear that compounds over time in joints that are already dealing with structural changes. Antioxidants from food help manage that process. They are not a cure for oxidative damage. They reduce the rate at which it accumulates.
One practical note on preparation. Raw or lightly cooked greens retain more of the active compounds than heavily processed or overcooked versions. A handful of spinach in a smoothie, arugula as a salad base, lightly sauteed kale with olive oil, all of these preserve what you are actually after. Boiling until grey is less useful.
You do not need to eat a pound of greens a day. Consistent daily exposure, even a modest amount, is more valuable than occasional large servings with nothing in between.
Why do berries belong on the anti-inflammatory foods list?
Blueberries, strawberries, raspberries, cherries. The thing that puts all of these in the same conversation is anthocyanins, a class of flavonoid that gives berries their color and does measurable work on inflammation.
Anthocyanins inhibit the COX-2 enzyme. If that sounds familiar, it is because COX-2 is the same pathway targeted by many over-the-counter anti-inflammatory medications. The effect of food is milder and more gradual than that of medication. But it is real, it accumulates with consistent consumption, and it comes without the gastrointestinal side effects that chronic NSAID use can produce in older adults.
Tart cherries deserve a separate mention. The research on tart cherry juice, specifically the tart variety rather than the sweet, shows reductions in inflammatory markers and muscle soreness following physical activity. That post-activity recovery piece is worth paying attention to.
A few practical notes. Fresh, frozen, and dried berries all retain meaningful levels of anthocyanins. Frozen is often more practical and significantly less expensive, particularly outside of peak season. If you are using dried berries, check the label; many commercially dried fruits have added sugar that works against what you are trying to accomplish.
Berries also happen to be one of the most accessible additions on this list. Most people already eat them occasionally. The shift is from occasional to consistent. That is a smaller ask than it might sound.
What does olive oil do for joint inflammation?
Extra virgin olive oil contains a compound called oleocanthal. Oleocanthal inhibits the COX-1 and COX-2 enzymes, which are the same pathways targeted by non-steroidal anti-inflammatory drugs. It was identified as a COX inhibitor in 2005 when researchers noticed that fresh extra virgin olive oil produced the same throat sensation as liquid ibuprofen.
The mechanism is real. The effect is dose-dependent and cumulative, not acute. Oleocanthal works over weeks and months of consistent use, not in the hours after a single meal. Managing expectations here matters. This is not a replacement for medication when you need it. It is a consistent background contribution to a lower inflammatory baseline.
Two things worth knowing about form and quality. First, extra virgin is the relevant designation. Refined olive oils lose most of the oleocanthal during processing. Light olive oil, pure olive oil, and other refined versions do not carry the same benefit. Second, oleocanthal degrades with heat. Using extra virgin olive oil as a finishing oil on cooked vegetables or as the base for salad dressings preserves more of the active compound than using it as a high-heat cooking oil.
The most practical shift for most people is replacing whatever oil they currently use most often with extra virgin olive oil. That one substitution, done consistently, is more useful than adding olive oil on top of an existing pattern that includes a lot of refined seed oils.
Is turmeric actually helpful for knee pain?
The honest answer is: probably yes, with some important caveats.
The active compound in turmeric is curcumin. Curcumin has well-documented anti-inflammatory properties in laboratory research and has been studied in several clinical trials involving adults with knee osteoarthritis. Meta-analyses of those trials show meaningful improvements in self-reported pain and physical function compared to placebo. The effect sizes are modest but consistent across studies.
The caveats matter. Study quality varies considerably. Many trials use concentrated curcumin supplements rather than culinary turmeric, which contains curcumin at much lower levels. And curcumin has a bioavailability problem: it absorbs poorly on its own. The body processes and eliminates it quickly before much of it reaches circulation.
The practical solution to the bioavailability issue is straightforward. Combining turmeric with black pepper significantly increases absorption. Black pepper contains piperine, a compound that inhibits the metabolic pathway that breaks curcumin down before it can be absorbed. Studies suggest piperine increases curcumin bioavailability by up to 2,000 percent. Cooking with turmeric and black pepper together is the most accessible way to take advantage of that interaction.
Where does this leave turmeric on the list? The research is encouraging rather than definitive. It is not at the level of omega-3s, where the evidence is deep and consistent. But it is a reasonable addition to an anti-inflammatory eating pattern, particularly when used in cooking alongside a fat source, which also aids absorption.
Add it to cooking. Use it with black pepper. Keep expectations proportionate to what the evidence actually supports.
Why does ginger show up in joint health research?
Ginger has been used for joint pain across a number of traditional medicine systems for centuries. The reason it keeps showing up in modern research is that the active compounds, gingerols and shogaols, have measurable effects on inflammatory pathways that are directly relevant to knee osteoarthritis.
Specifically, gingerols and shogaols inhibit the production of inflammatory cytokines and have shown analgesic properties in several small trials. A 2015 meta-analysis by Bartels et al. looked at the pooled evidence from randomized placebo-controlled trials and found statistically significant reductions in pain and disability in adults with knee osteoarthritis who consumed ginger compared to placebo (Bartels et al., 2015).
The honest framing on effect size: modest. Ginger is not a powerful standalone intervention. It is a useful contributor to an overall anti-inflammatory eating pattern, and the research supports including it on that basis.
Practically, ginger is one of the more versatile items on this list. Fresh ginger, grated for cooking, adds flavor alongside its function. Dried ginger works in baking and spice rubs. Steeped as tea, it is one of the most accessible daily habits on the list, particularly for adults who find the idea of dietary change overwhelming. A cup of ginger tea in the morning is a small, consistent, zero-disruption addition that most people can sustain.
Fresh and dried ginger both contain the active compounds, though fresh ginger has higher concentrations of gingerols specifically. Either form is a reasonable choice depending on what fits your cooking habits.
What role do nuts and seeds play in reducing inflammation?
Nuts and seeds earn their place on this list through two different mechanisms, and understanding both helps you make better choices about which ones to prioritize.
The first mechanism is omega-3 fatty acids. Walnuts, flaxseeds, and chia seeds are the plant kingdom’s most concentrated sources of ALA, an omega-3 fatty acid that the body can convert to EPA and DHA. The conversion rate is limited compared to getting EPA and DHA directly from fatty fish, somewhere between five and fifteen percent, depending on the individual. That limitation is worth knowing about honestly. Plant-based omega-3s are a useful contribution to overall intake, not a direct substitute for fatty fish.
The second mechanism is vitamin E. Almonds, sunflower seeds, and hazelnuts are high in vitamin E, a fat-soluble antioxidant that reduces oxidative stress associated with chronic inflammation. For adults managing ongoing joint concerns, oxidative stress is a real contributor to the daily experience of discomfort. Vitamin E works on that piece specifically.
Walnuts are worth highlighting because they sit at the intersection of both mechanisms. They are the highest ALA source among tree nuts, and they also carry meaningful antioxidant compounds. A small handful of walnuts as a daily snack is one of the simpler additions on this list and one of the more efficient ones in terms of what you get per serving.
One practical note on form. Whole nuts and seeds retain their nutritional profile better than heavily processed versions. Nut butters made with just the nut and nothing else are a reasonable alternative. Products with added oils, sugar, or hydrogenated fats work against what you are trying to accomplish.
How do you put anti-inflammatory eating into practice without overhauling your diet?
Seven foods are not a diet. It is a direction.
Anti-inflammatory eating is not a protocol with rules you follow perfectly or abandon entirely. It is a pattern of consistent choices that, over weeks and months, shifts your body’s baseline inflammation in a direction that makes daily movement more manageable. The goal is not perfection. It is a gradual accumulation of small, sustainable additions.
The foods that work against that direction are worth knowing about briefly. Refined sugar, processed seed oils, ultra-processed products, and refined carbohydrates consistently appear in research as drivers of systemic inflammation. You do not need to eliminate them entirely. Reducing their frequency and replacing them gradually with foods from this list is a more realistic and more durable approach than any version of starting over from scratch.
A practical starting point. Pick one food from the seven and add it to something you are already eating this week. Not all seven. One. Sardines on the crackers you already buy. A handful of walnuts alongside the afternoon snack you already have. Frozen blueberries in the yogurt you already eat. One consistent addition over two weeks builds more than seven simultaneous changes that last four days.
From there, add another. Then another. The pattern builds itself if you give it enough time and enough grace.
This is one pillar of three. Movement and Mindfulness work alongside it. None of the three works as well alone as all three do together, and that combination is exactly what M3 is built on.
Before making significant dietary changes, particularly if you are managing other health conditions, consult your physician. Nutritional guidance in this post is educational.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Wrap-up: The best anti-inflammatory foods for knee pain
Food is not the whole answer. Anyone who tells you otherwise is selling something.
But it is one real piece of a picture that most people managing knee pain have never been given completely. The joint gets all the attention. The environment the joint is operating in gets almost none. What you eat is part of that environment, and it is one of the few parts you can change starting today without waiting for an appointment, a prescription, or a program.
The seven foods on this list work by lowering the baseline inflammation your knees are working against every single day. Not dramatically. Not overnight. Gradually, cumulatively, in a way that compounds over weeks and months of consistent choices.
Fatty fish for the omega-3s that modulate your inflammatory response at the cellular level. Leafy greens for the vitamin K and antioxidants that support cartilage metabolism. Berries contain anthocyanins that inhibit the same enzyme pathways as common anti-inflammatories. Olive oil contains oleocanthal that does similar work more gently over time. Turmeric and ginger for their cumulative contributions to the same direction. Nuts and seeds provide plant-based omega-3s and vitamin E that fill in what the others do not cover.
One food this week. Then another. That is the whole instruction.
Movement works alongside this. So does how you manage the mental load of living with chronic joint concerns. All three pillars together are what produce lasting change. This post covers one of them.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Frequently Asked Questions
What foods make knee inflammation worse?
Refined sugar, processed seed oils, and ultra-processed products are the most consistent drivers of systemic inflammation in the research. Refined carbohydrates, alcohol consumed in large quantities, and trans fats also appear regularly as contributors. You do not need to eliminate all of these overnight. Reducing their frequency while gradually increasing the foods on the anti-inflammatory list is a more durable approach than any version of starting over completely.
How long does it take for anti-inflammatory foods to work?
Most research on dietary inflammation patterns looks at outcomes over eight to twelve weeks of consistent intake. You are unlikely to notice a dramatic shift in the first week. What most adults report after four to six weeks of consistent anti-inflammatory eating is a subtle reduction in the daily baseline of discomfort, less morning stiffness, and joints that feel somewhat more responsive to movement. The effect is gradual and cumulative, not acute.
Do I need a special diet for knee pain?
No. What the research supports is a directional shift in eating patterns, not a specific named diet or a set of rigid rules. Adding more of the seven foods covered in this post, reducing the foods that consistently drive inflammation, and doing both consistently over time is the whole approach. It fits inside whatever eating pattern you currently have rather than replacing it.
Can food changes reduce knee swelling?
Acute swelling following injury or a flare needs medical attention, and food choices are not the right intervention there. Chronic, low-grade joint inflammation that contributes to ongoing discomfort and stiffness is a different situation. Consistent anti-inflammatory eating has been shown to reduce inflammatory markers in the blood over time, which affects the chronic inflammatory component of knee osteoarthritis. That is not the same as reducing acute swelling, and the distinction matters.
Is turmeric or ginger better for knee pain?
They work through related but different mechanisms, and the research supports including both rather than choosing between them. Turmeric via curcumin has broader anti-inflammatory evidence, but a bioavailability limitation that is addressed by combining it with black pepper. Ginger, via gingerols and shogaols, has more specific trial evidence in knee osteoarthritis populations from the Bartels et al. 2015 meta-analysis. Used together in cooking, they contribute to the same overall direction without duplicating each other.
What is the one dietary change that makes the biggest difference for knee pain?
Replace refined seed oils with extra virgin olive oil as your primary cooking and finishing oil. It addresses the inflammatory baseline from two directions simultaneously: reducing a known driver of inflammation and adding oleocanthal, which inhibits the same COX pathways as common anti-inflammatory medications. It is also one of the most seamless substitutions on the list because it replaces something you are already using rather than adding something new.
References
Bartels, E. M., Folmer, V. N., Bliddal, H., Altman, R. D., Juhl, C., Tarp, S., Zhang, W., & Christensen, R. (2015). Efficacy and safety of ginger in osteoarthritis patients: A meta-analysis of randomized placebo-controlled trials. Osteoarthritis and Cartilage, 23(1), 13–21. https://doi.org/10.1016/j.joca.2014.09.024
Beauchamp, G. K., Keast, R. S. J., Morel, D., Lin, J., Pika, J., Han, Q., Lee, C.-H., Smith, A. B., & Breslin, P. A. S. (2005). Phytochemistry: Ibuprofen-like activity in extra-virgin olive oil. Nature, 437(7055), 45–46. https://doi.org/10.1038/437045a
Burdge, G. C., & Calder, P. C. (2005). Conversion of alpha-linolenic acid to longer-chain polyunsaturated fatty acids in human adults. Reproduction, Nutrition, Development, 45(5), 581–597. https://doi.org/10.1051/rnd:2005047
Calder, P. C. (2013). Omega-3 polyunsaturated fatty acids and inflammatory processes: Nutrition or pharmacology? British Journal of Clinical Pharmacology, 75(3), 645–662. https://doi.org/10.1111/j.1365-2125.2012.04374.x
Hewlings, S. J., & Kalman, D. S. (2017). Curcumin: A review of its effects on human health. Foods, 6(10), Article 92. https://doi.org/10.3390/foods6100092
Minihane, A. M., Vinoy, S., Russell, W. R., Baka, A., Roche, H. M., Tuohy, K. M., Teeling, J. L., Blaak, E. E., Fenech, M., Vauzour, D., McArdle, H. J., Kremer, B. H. A., Sterkman, L., Vafeiadou, K., Benedetti, M. M., Williams, C. M., & Calder, P. C. (2015). Low-grade inflammation, diet composition and health: Current research evidence and its translation. British Journal of Nutrition, 114(7), 999–1012. https://doi.org/10.1017/S0007114515002093
Seeram, N. P., Momin, R. A., Nair, M. G., & Bourquin, L. D. (2001). Cyclooxygenase inhibitory and antioxidant cyanidin glycosides in cherries and berries. Phytomedicine, 8(5), 362–369. https://doi.org/10.1078/0944-7113-00053
Shea, M. K., & Booth, S. L. (2016). Concepts and controversies in evaluating vitamin K status in population-based studies. Nutrients, 8(1), Article 8. https://doi.org/10.3390/nu8010008
A client I worked with, I’ll call her Carol, stopped walking entirely for six months. Not because her doctor told her to. Because she was convinced that every step was grinding her knee down a little more. By the time she found me, she had gained twelve pounds, her knee was stiffer than it had been before she stopped, and she was more afraid of movement than ever.
Carol is not unusual. The fear makes sense. When something hurts when you do it, stopping feels like the obvious answer. If you have been wondering whether it is okay to walk with knee pain, you are not alone. And the answer matters more than the generic advice you have probably already received.
For most adults over 55 with chronic knee pain, it is the wrong one.
KEY TAKEAWAY
For most adults with knee pain, walking is not only safe — it is one of the most effective things you can do. The American College of Rheumatology classifies exercise as first-line management for knee osteoarthritis (ACR/AF, 2019). A Cochrane review of 54 trials confirmed that exercise improves function and reduces discomfort in adults with knee OA (Fransen et al., 2015). The key is how you start.
Here is what the research says: when to pump the brakes and see a doctor, and the smallest safe starting point for someone who has been avoiding movement for months.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Table of Contents
Is walking safe when your knees already hurt?
For most people, yes. But let me be more specific than that, because the answer depends on what kind of pain you are dealing with.
There is a difference between chronic aching and acute injury. Chronic aching is the dull, ongoing discomfort that has been showing up for weeks or months without a clear cause. No fall. No impact. It just arrived and stayed. That is the pattern most adults over 55 come to me with, and that is the pattern this post addresses.
Acute injury is different. Sharp, sudden pain after a fall or impact, visible swelling, or a feeling that your knee might give way are signals to stop and see your doctor before doing anything else. Those need imaging and clinical assessment. Do not walk through those.
If you are in the chronic aching category and you are wondering whether every step is making things worse, the research has a clear answer. It is not. For most adults managing knee osteoarthritis or age-related joint changes, walking done correctly does not damage the joint further. It helps it. I cover exactly why that is in the next section.
One more thing before we move on. Nothing in this post is medical advice. If you are uncertain whether your situation is safe to work with, start with your physician. That conversation costs you nothing and rules out anything that needs attention before you begin. If you want to understand more about what is actually causing your knee pain during walking, I covered that in detail in why your knees hurt when you walk.
What does the research actually say about walking and knee pain?
More than most people expect, and it is clearer than the generic advice you have probably been given.
The American College of Rheumatology and the Arthritis Foundation classify exercise, including walking, as first-line management for knee osteoarthritis (ACR/AF, 2019). Not a supplement to treatment. Not something to try if other things do not work. First line. That is the standard clinical recommendation, and it has been for years.
The research behind that recommendation is substantial. Fransen et al. (2015) analyzed 54 randomized controlled trials and found that land-based exercise consistently improved function and reduced discomfort in adults with knee osteoarthritis. Fifty-four trials. That is not a promising early signal. That is a settled body of evidence.
Here is the part that surprises most of my clients. The people who kept moving, within their capacity, were the ones who stayed more capable over time. Not the ones who rested more. Not the ones who waited until the pain was gone. The ones who found a level of movement they could sustain and stuck with it.
There is a physiological reason for this. Your knee joint depends on movement to circulate synovial fluid, its built-in lubricant. When you stop moving, that fluid stagnates. Stiffness increases. The muscles that surround and support the joint continue their natural decline after 55, regardless of whether you are in pain or not. The joint ends up absorbing a load it was never designed to handle alone.
Rest has a place. Acute injury, significant swelling, and post-surgical recovery, those call for rest. Chronic, ongoing aching during a regular walk is a different situation entirely. The research points in one direction. Movement is the answer, not more time on the couch.
When should you stop walking and see a doctor?
I want to be direct about this because getting it wrong in either direction has real consequences.
If you experience any of the following, stop walking and see your doctor before you do anything else.
Sharp, sudden pain after a fall or impact.
Visible swelling in or around the knee joint.
A feeling that your knee might give way or buckle underneath you.
Pain that is significantly worse than your usual baseline, not just a bad day, but a meaningful shift in what you are feeling.
Any new symptom that has not been part of your usual pattern.
Those signals are your body asking for clinical attention. Do not walk through them and do not use this post, or any post, as a reason to delay that conversation.
Post-surgical situations deserve a separate note. If you have had knee surgery recently, your return-to-activity timeline comes from your surgeon, not from general guidance about walking and knee pain. Follow their protocol.
For everyone else, the question to ask yourself is this. Is what I am feeling a chronic, ongoing ache that has been present for weeks or months without a clear acute event behind it? If yes, you are in the group the research consistently supports. Movement, done correctly, is the right direction.
You know your body. If something feels different from your usual ache, that difference is worth a conversation with your doctor. That instinct is good information. Use it.
How do you start walking safely when knee pain has been stopping you?
This is where most programs lose the adults I work with. They assume you already have a walking habit and ask you to walk thirty minutes three times a week, starting on day one. For someone who has been avoiding movement for months out of fear or pain, that is not a starting point. That is a finish line.
Two minutes is a real starting point. Not a warm-up. An actual session.
I know that sounds almost embarrassingly small. It is not. The goal in the first week is not fitness. It is not even progress in the traditional sense. It is showing your joint that the movement is safe. You are building a signal, not a habit yet. The habit comes later, once the signal is established.
Four practical things to get right from the beginning.
Duration. Start at two to three minutes. Add one to two minutes every few days, not every day. Let your joint tell you when it is ready for more.
Surface. Flat and even with some give. Packed dirt, a rubberized track, or a treadmill is more forgiving than hard concrete. Pick the surface you will actually use over the one that sounds ideal.
Pace. Comfortable. Conversational. If you cannot hold a short conversation while walking, you are moving too fast for this stage.
Footwear. Cushioned, supportive sneakers with a firm midsole. Not fashion. Not flat shoes. Not whatever is nearest the door. This is the one equipment investment that actually moves the needle.
Here is the most important thing I can tell you about tracking your progress. How your knees feel two to four hours after a walk is your real data point, not how they feel mid-walk or immediately after. Discomfort that ramps up hours later means shortening the next session. Discomfort that fades or stays flat means you are working at the right level. That post-session window tells you more than anything else.
The 3-Minute Knee Test gives you a structured 7-day tracking sheet built around exactly this approach. You try it once. You track how your body responds. You have real data before you commit to anything more.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
What else makes a difference when you walk with knee pain?
The starting point matters most. But once you are moving consistently, a few other factors influence how your knees respond.
Consistency beats intensity every time. Two minutes every day builds joint tolerance faster than twenty minutes twice a week. Your joint responds to pattern, not volume. The adults I work with who make the most progress early are not the ones who push hardest on good days. They are the ones who show up on the ordinary days when nothing feels particularly inspiring.
Morning stiffness is real, and it has a reason. Synovial fluid thickens overnight from inactivity. The first few steps after waking can feel worse than any walk you take later in the day. A short warm-up before you head out, even just walking slowly around the house for a minute or two, redistributes that fluid and makes the actual walk feel considerably different.
What you eat affects how your knees feel on a walk. Chronic joint discomfort has an inflammatory component. Foods that drive systemic inflammation, particularly refined sugar, processed seed oils, and ultra-processed products, raise your baseline. Your knees start every walk already more sensitized than they need to be. Anti-inflammatory foods, including fatty fish, leafy greens, olive oil, and berries, work in the other direction. They will not reverse structural joint changes. But lower baseline inflammation often means the same walk produces less discomfort.
Worn-out shoes are a silent contributor. Most people replace walking shoes far less often than they should. A midsole that has compressed visibly is no longer absorbing impact the way it was designed to. If your shoes are more than a year old and you walk regularly, they are probably past their useful life for joint protection purposes.
None of these factors matters as much as simply starting. The best surface is the one you will actually walk on. The best time is the one you will actually keep. Get the basics right first, then layer these in as you build.
Wrap-up: Is it safe to walk with knee pain?
For most adults over 55 with chronic knee pain, yes. Not recklessly. Not by pushing through signals your body is sending you. But with the right approach, at the right starting point, walking is not something to be afraid of.
Carol eventually got back to walking. She started with two minutes. She tracked how her knees felt two to four hours after each session. She added time slowly. Eight weeks later, she was walking twenty minutes most mornings, and her knee was less stiff than it had been in two years. She told me the hardest part was giving herself permission to start that small.
That is the part most people skip. They wait until they feel ready for a real walk. A real walk is whatever you can do today without paying for it tomorrow. For some people, that is two minutes. That is enough to begin.
The research is on your side. The clinical guidelines are on your side. Thirty years of working with adults in exactly your situation tells me the same thing. Movement done correctly is not what is hurting your knees. Avoiding it is.
Start where you are. Track what happens. Let your body show you what it can do.
Ready to Find Out What Your Body Can Do?
It takes less than 3 minutes. No gym. No equipment. Just a simple test that shows you if your body can do more than it’s been telling you.
M3 is a behavioral wellness coaching program. It is not medical treatment and does not replace advice from your physician. Consult your doctor before beginning any new movement or nutrition program.
Frequently Asked Questions
Can walking make knee pain worse?
It can, if the approach is wrong. Going too far too fast, walking on hard surfaces in unsupportive shoes, or pushing through sharp pain during a session are the most common ways walking backfires. The approach matters as much as the activity itself. Short sessions, manageable pace, and attention to how your knees feel two to four hours after are what keep walking in the helpful column rather than the harmful one.
How far should I walk if my knees hurt?
Start with two to three minutes and build from there. Distance is the wrong measure at the beginning. Duration is more useful, and even that is secondary to how your joint responds post-session. Add one to two minutes every few days when your post-session feedback tells you the current level is manageable. Most adults find they are walking fifteen to twenty minutes consistently within six to eight weeks of starting at two minutes.
What type of walking surface is best for knee pain?
Packed dirt trails, rubberized tracks, and treadmills are the most forgiving surfaces for adults managing knee pain. They absorb more impact than concrete or asphalt. Hard flat pavement is the least forgiving option. That said, the best surface is the one you will actually use consistently. A daily walk on concrete beats an occasional walk on the perfect trail every time.
When should I see a doctor about knee pain during walking?
See your doctor if you experience sharp, sudden pain after a fall or impact, visible swelling, a feeling that your knee might give way, or pain that is meaningfully worse than your usual baseline. Ongoing chronic aching without a clear acute cause is generally not an emergency, though a physician visit before starting any new movement routine is always a reasonable first step. When in doubt, get it checked.
Is it better to walk every day or rest some days when you have knee pain?
For chronic knee pain, daily short walks tend to outperform longer walks with rest days in between. Your joint responds to consistent movement. Synovial fluid circulates better, stiffness reduces more reliably, and the habit builds more durably when movement is part of everyday life rather than an event that happens a few times a week. If a particular day produces more discomfort, shorten the session rather than skipping it entirely.
Does walking speed matter when you have knee pain?
At the beginning, no. Comfortable and conversational is the right pace for the first several weeks. If you cannot hold a short conversation while walking, you are moving too fast for this stage. Speed becomes relevant later, once you have established a consistent daily habit and your joint has built some tolerance. For now, showing up matters more than how fast you get there.
References
American College of Rheumatology/Arthritis Foundation. (2019). Guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis & Rheumatology, 72(2), 149-162.
Fransen, M., McConnell, S., Harmer, A. R., Van der Esch, M., Simic, M., & Bennell, K. L. (2015). Exercise for osteoarthritis of the knee: A Cochrane systematic review. British Journal of Sports Medicine, 49(24), 1554-1557.